Life Extension Magazine®
The Multiple Health Benefits of Coenzyme Q10 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| By Saul Kent President Life Extension Foundation Could you use more energy? Most lO-year-olds are bursting with energy. At age 30 most of us still have plenty of energy. By 40 we're beginning to slow down, but experience allows us shortcuts to reduce our energy needs. However by age 60, our energy levels are so depleted that even the wisdom of our years can't make up for our decline. If we make it to 80, we're just a shadow of our former selves. And if we reach 100, we're thrilled just to be alive. It's not just our body as a whole that needs energy it's our individual cells as well. Our brain cells need energy to think, our heart cells need energy to keep our blood circulating, our lung cells need energy to process oxygen, our kidney cells need energy to excrete waste, our bone and muscle and cells need energy for structure and strength, and our immune cells need energy to fight off invading organisms. Depletion of EnergyAlthough most diseases aren't caused by defects in the generation of energy, they're all characterized by energy depletion. Cancer stroke, heart disease, diabetes, and Alzheimer's disease are different in their origin and expression, but they have one thing in common: depletion of the energy-generating capacity of essential cells. Energy depletion caused by diseases produces feelings of weakness, lassitude, depression, despair and hopelessness. Its endpoint is death. As you know such feelings don't just come from overt diseases. Lack of energy is one of the most common complaints in people of all ages Whether reduced energy is caused by subclinical disease states, unpleasant or traumatic experiences, the "normal" ups and downs of life, or the ravages of aging, the feelings are the same. No one likes to feel weak. No one likes to be unable to do things they need to do. No one likes to see life as dark, colorless and unexciting. No one likes pain and suffering. And no one likes to feel as if their life is slipping away from them. The Central Failure In Human LifeThe central failure in human Iife is weakness: lack of strength; lack of purpose; lack of character; and lack of will. The appropriate reaction to weakness and feelings of inadequacy is to build oneself up, but all too often people strive to tear others down, or to rely on others for their self esteem. The results in social terms have been personal conflict, estrangement, war, and victimization. Effects On Health And Medical CareThe effects on health and medical care have been reliance on doctors to "cure" us rather than taking responsibility for our own lives, the focus on the treatment of diseases rather than their prevention, and the attempt to destroy our enemies (viruses, bacteria, and other organisms) rather than to maintain our youth, become stronger, and build up our defenses. A tragic example of the failure of our medical system is the story of Coenzyme Q, (CoQ10 )- an essential component of our energy-generating system -- whose structure and function was discovered in the United States in the late 1950s, but whose role in health care has been almost totally ignored by the U.S. medical establishment, except for the heroic efforts of Dr. Karl Folkers of the University of Texas at Austin. The Discovery Of Coenzyme Q10 In 1956, scientists at the University of Wisconsin under Dr. David E. Green isolated a crystalline yellow compound from beef heart mitochondria (the energy factories of the cell). They gave a few milligrams of this sample to Dr Folkers, who was head of a biochemical research team at Merck Sharp And Dohme Research Laboratories in Rahway, New Jersey. Dr. Folkers and his coworkers at Merck determined that the chemical structure of CoQ is 2,3-dimethoxy-5-methly-6-decaprenyl-1,4-benzoquinone. This structure was revealed at the International Congress on Biochemistry in Vienna in 1958 and published that year in the Journal of the American Chemical Society (60:4752). FIGURE 1
Concentration And Biosynthesis Of CoQCoQ is found in high concentrations (bound to three different proteins) in the heart, liver kidney, and pancreas. The total body content of CoQ has been estimated to be 0.5-1.5 grams. About 50% of the CoQ in the body is found within the mitochondria, where energy is generated on a continuous basis, and where CoQ has three major functions: to help several mitochondrial enzymes convert dietary nutrients (in the presence of oxygen) into the energy "currency" of the body ATP (Adenosine Triphosphate); to help quench some of the free radicals generated in the energy making process; and to help protect the integrity of the mitochondrial membrane. CoQ levels have been shown to be well below normal in patients with a wide variety of diseases including heart disease, cancer and muscular dystrophy, as well as in normally aging people. One likely reason for these age and disease-related declines in CoQ may be the complexity of the process by which CoQ is synthesized within the body. CoQ is biosynthesized from the amino acids phenylalanine and tyrosine with the help of at least eight vitamins and trace elements (figure 2) all of which have vital biochemical functions in the body in addition to the manufacture of CoQ. Anyone with deficiencies of any of these nutrients is likely to become deficient in CoQ. When you add the aging-related breakdown of mitochondrial function which includes unrepairable DNA mutations - it's no wonder that our bodies hunger so much for this remarkable, life-enhancing nutrient. Figure 2The steps in the sequence for the
|
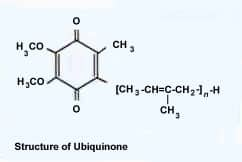 Their discovery was given the name Coenzyme Q10 because it has the biochemical role of a coenzyme (it aids in the action of enzymes) because the letter Q is the first letter of the word quinone, and because it has 10 isoprenoid units on its side chain (figure 1). Dr R.A. Morton and associates at the University of Liverpool in England named CoQ ubiquinone in their 1958 paper in Nature (182:1764) because it is found in virtually every cell of the body.
Their discovery was given the name Coenzyme Q10 because it has the biochemical role of a coenzyme (it aids in the action of enzymes) because the letter Q is the first letter of the word quinone, and because it has 10 isoprenoid units on its side chain (figure 1). Dr R.A. Morton and associates at the University of Liverpool in England named CoQ ubiquinone in their 1958 paper in Nature (182:1764) because it is found in virtually every cell of the body.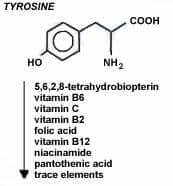 The Japanese Take The Lead
The Japanese Take The Lead| Possible Therapeutic Mechanisms of Coenzyme Q10 Cardiovascular Disease |
| 1. Correction of CoQ deficiency state. |
| 2. Direct free radical scavenger via semiquinone species. |
| 3. Direct membrane stabilizing activity due to phospholipid protein interactions. |
| 4. Correction of mitochondrial "leak" of electrons during oxidative respiration. |
| 5. Induction of DT diaphorase. |
| 6. Possible effects on prostaglandin metabolism. |
| 7. Inhibition of intracellular phospholipases. |
| 8. Preservation of myocardial Na+- K+ ATPase activity. |
| 9. Stabilization of integrity of Ca+2dependent slow channels. |
Italian Multicenter Study
The Italian study looked at CoQ as an adjunct to conventional drugs in 2,664 heart patients in 173 clinical centers over a 3-month period. The daily dosage of CoQ was 50-150 mg daily with the majority of patients (78%) receiving 100 mg/day. The patients in the study were all rated Class II and III (moderately ill) according to a rating scale based upon the guidelines formulated by the New York Heart Association (NYHA) regarding the symptoms associated with congestive heart failure.
The results showed improvement in virtually all functions measured in the CoQ-treated patients. The proportions of patients exhibiting significant improvement (of at least one point) in clinical symptoms was as follows (Tables 2 and 3): cyanosis 78.1%, edema 78.6%, pulmonary rate 77.8%, enlargement of liver 49.3%, jugular reflex 71.8%, dyspnoea 52.7%, palpitations 75.4%, sweating 79.8%, arrhythmias 63.4%, insomnia 66.8%, and vertigo 73.1%. They also found significant improvement in at least three symptoms in 54% of the patients, indicating major improvement in the quality of their lives.
The investigators summed up their results as follows:
"A significant reduction in blood pressure and heart rate, both in supine and sitting position, was observed in our study. These data confirm the results of a recent study in which CoQ, therapy led to a reduction in peripheral vascular resistance, resulting in a significant decrease in blood pressure. An inhibitory effect of CoQ10 on plasma catecholamine levels in heart failure has been recently reported. In our patients, the reduction in peripheral vascular resistance may be related to an inhibition by CoQ, of the sympathetic overactivity known to be present early in heart failure. The reduction in sweating and palpitations, reported by our patients may result from the same mechanism."
Table 2
Clinical Signs Assessment Results
| Description | Present at baseline(n) | Improved at least 1 point after 3 months of CoQ10 treatment (%) | Statistical signifiance of score variations* |
| Cyanosis | 675 | 78.67 | P<0.01 |
| Odema | 1764 | 78.06 | P<0.01 |
| Pulmonary Rates | 1752 | 77.85 | P<0.01 |
| Enlargement of liver area | 1285 | 49.26 | P<0.01 |
| Jugular reflux | 713 | 71.81 | P<0.01 |
Table 3
Clinical Symptoms Assessment Results
| Description | Present at baseline(n) | Improved at least 1 point after 3 months of CoQ10 treatment (%) | Statistical signifiance of score variations* |
| Dyspnoea | 2163 | 52.75 | P<0.01 |
| Palpitations | 1903 | 75.46 | P<0.01 |
| Sweating | 1044 | 79.79 | P<0.01 |
| Subjective arrhythima | 1143 | 63.43 | P<0.01 |
| Insomnia | 1597 | 62.87 | P<0.01 |
| Dizziness | 1282 | 73.13 | P<0.01 |
| Nocturia | 1541 | 53.67 | P<0.01 |
Treatment Of Hypertension With CoQ
We've been recommending CoQ to patients with cardiovascular disease for years with very good results. Most of these patients start taking CoQ in addition to the conventional drugs they are using. In many cases, they find that prolonged use of CoQ eliminates their need for such prescription drugs, A recent study of the use of CoQ in patients suffering from hypertension (high blood pressure) showed how CoQ can' help patients dispense with their drugs.
This study was conducted by scientists (including Karl Folkers) at the University of Texas at Austin. A total of 109 patients with hypertension were given a variable dose of from 75 to 360 mg/day of CoQ in addition to the existing drug regimen. The patients were followed closely with frequent clinic visits to record blood pressure and make the necessary adjustments in dosage. No side effects or drug interactions were found in any of the patients in the study.
Figure 3
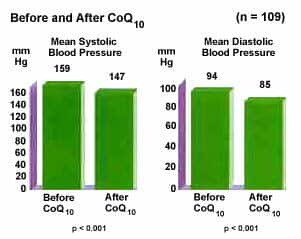 They found that mean systolic blood pressure improved from 159 to 147 and mean diastolic blood pressure improved from 94 to 85 (Figure 3). They also found that, as the patients' functional status and blood pressure improved, and there was a gradual decrease in the need far antihypertensive drugs. Thirty-seven percent of the patients were able to discontinue one drug, 11% discontinued two drugs, and 4% discontinued three drugs. The average time before stopping an anti- hypertensive drug was 4.4 months after starting CoQ, with 62% requiring 3 or more months (Figure 4).
They found that mean systolic blood pressure improved from 159 to 147 and mean diastolic blood pressure improved from 94 to 85 (Figure 3). They also found that, as the patients' functional status and blood pressure improved, and there was a gradual decrease in the need far antihypertensive drugs. Thirty-seven percent of the patients were able to discontinue one drug, 11% discontinued two drugs, and 4% discontinued three drugs. The average time before stopping an anti- hypertensive drug was 4.4 months after starting CoQ, with 62% requiring 3 or more months (Figure 4).
 Figure 4
Figure 4
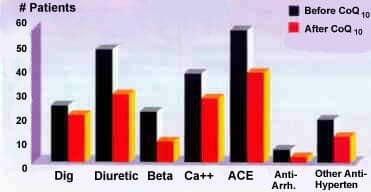 Figure 4
Figure 4They concluded that:
"CoQ, a both remarkably safe and cost effective and should be considered among the initial therapeutic modalities alongside such fundamental recommendations as diet exercise and stress reduction and should certainly be considered prior to embarking upon on escalating course of pharmacologic interventions with all of their well established medical and economic hazards."
Interestingly, the Texas scientists found that the most effective way of raising blood levels of CoQ in patients was to give it with a fat containing food (usually peanut butter), which "more than doubled the blood CoQ level on any given dosage." This is not surprising because CoQ is a fat-soluble nutrient that assimilates better in the presence of fat. For this reason, The Foundation now offers CoQ in oil-based, soft-gel capsules, which maximizes its bioavailability within the body.
The Bioavaliability of CoQ
Recent studies at the Royal Danish School of Pharmacy in Denmark have demonstrated that "CoQ in soy bean oil in soft gelatine capsules has higher bioavailability than CoQ formulated with other inert substances." These studies compared CoQ in dry powder form (in capsules) and in tablets with various oil-based formulations of CoQ. It is on the basis of these studies that we now offer CoQ in the same soy-bean-oil formula shown in these studies to produce optimal absorption of CoQ into the body. For further information about this product, call 1-800-64414440 or you can order CoQ10 On-line.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun