Life Extension Magazine.

Neutralize a Harsh Reality
Elevated ApoB increases cardiovascular disease risks. ApoB blood tests provide a more complete picture of cardiovascular risk and allow for corrective actions before a cardiovascular event strikes.
Scientifically reviewed by: Gary Gonzalez, MD, in May 2026. Written by: William Faloon.

Atherosclerosis is one of the leading causes of morbidity and mortality in individuals over the age of 65.1,2
The medical literature shows that atherosclerosis underlies the majority of heart disease, cerebrovascular disease, and peripheral arterial disorders.1,2
Coronary artery disease,3 driven by atherosclerosis, is the leading cause of cardiovascular death in older adults.3-5
Complications include heart failure4,6 and arrhythmia,7,8 which are major contributors to morbidity, loss of independence, and impaired quality of life.9
The prevalence of coronary atherosclerotic lesions in people just over 50 years old may be extremely high.10
A study on over 2,000 people living in South Florida, whose average age was 53, showed that about half had plaque in their coronary arteries.10
The question is what can be done to halt and partially reverse this?
Arterial clogging begins early in life but does not usually manifest symptomatically until later years.11 By that time, there is systemic arterial damage that often requires aggressive steps to correct.
Based on current evidence, some physicians are aggressively lowering the recommended levels of a major cause of atherosclerosis in their patients.
This risk factor is called apolipoprotein B (ApoB).12
There is no debate that elevated ApoB increases cardiovascular disease risks.
I wrote about this in the June 2019 issue of Life Extension Magazine®, and we added ApoB to our comprehensive blood test panels long ago.13
The consensus is that optimal ApoB ranges are under 90 mg/dL for primary prevention and below 60 mg/dL for higher-risk patients.13,14
Some argue ApoB recommendations should be even lower, especially for high-risk individuals. About half of people over age 50 may have coronary atherosclerotic lesions…and thus are potentially high-risk individuals, especially if they live long enough.
Most readers of Life Extension Magazine® practice healthy longevity via diet, exercise, supplements, and appropriate use of medications. It is also important to reduce ApoB blood levels if elevated.
This editorial succinctly describes differing views of the published clinical data in an effort to identify ideal ApoB levels to protect against cardiovascular diseases.
There has been a long-standing debate regarding the atherogenic properties of elevated cholesterol.
There is also a debate about the value of ApoB testing, the results of which many argue can be inferred from LDL cholesterol results. (Some believe that those with low LDL are also likely to have low ApoB.)
ApoB is a protein found on the surface of all non-HDL-carrying lipoproteins in the blood, such as LDL and VLDL. ApoB is a critical element that makes lipoprotein particles atherogenic, meaning they can cause atherosclerosis.12,15
ApoB-containing particles can enter the walls of arteries. Once inside, they tend to get stuck, especially in areas where the artery wall is damaged or inflamed. This trapping is a critical step in the development and progression of atherosclerosis.
The more ApoB-containing particles present in the blood, the more likely they are to accumulate in the artery wall, leading to the buildup of plaques which can grow, become inflamed, and eventually block blood flow, rupture, or erode, causing heart attacks or strokes.15
What this means is that while the effects of elevated cholesterol have been fiercely debated, the insidious role of elevated ApoB is often overlooked.
The Benefits of Lowering ApoB

Clinical trial data and ongoing studies indicate that for those at high risk of cardiovascular disease, achieving very low ApoB using newer lipid-lowering agents is feasible and generally safe, but long-term outcome data remains limited.16,17 We have much more data when it comes to reducing LDL to very low levels.14
Interventional data that targets lowering ApoB levels is limited. But there are some studies using PCSK9 inhibitors, which are medications primarily recommended for high cardiovascular risk patients who are not achieving lipid targets with statin therapy alone.14
Two randomized controlled trials found that adding the PCSK9 inhibitors evolocumab (Repatha®) or alirocumab (Praluent®) to statin therapy significantly reduced ApoB levels, achieving mean ApoB concentrations roughly below 50 mg/dL.14,16,17
These studies have demonstrated that rigorous lipid-lowering with these drugs may have a small effect at reducing major adverse cardiovascular events in high-risk populations without a safety concern. However, there is a lack of long-term outcome data specifically for sustaining ApoB at this low level.
Can Atherosclerosis be Reversed?

Aggressively lowering ApoB and/or LDL in people with elevated atherogenic lipids is more effective at reducing the lifetime cardiovascular risk when initiated during young adulthood rather than later in life. This is because early exposure drives a greater burden of atherosclerosis and adverse cardiovascular events over decades.18
The degree of plaque regression is proportional to the extent of LDL- and ApoB-lowering, as demonstrated in intravascular ultrasound studies and clinical trials.19,20 Complete regression is not consistently achieved in all patients, especially those with established, advanced disease.
A meta-analysis of randomized controlled trials in patients with high cardiovascular risk or atherosclerosis compared intensive lipid‑lowering therapy achieving LDL cholesterol <40 mg/dL with therapy achieving higher LDL levels (>40 mg/dL). Very low LDL levels were associated with fewer major adverse cardiovascular events and no increase in serious adverse events.21
However, not all patients treated with statins to achieve low LDL levels (<70 mg/dL), or even the very low levels (<40 mg/dL) achievable with a combination of statins and a PCSK9 inhibitor, will experience plaque regression. This may be due, in part, to other atherogenic factors such as elevated glucose-A1C and C-reactive protein (CRP).22,23
Gaining control over all atherogenic risks is the best we can do to mitigate the risk of cardiovascular disease…today’s leading cause of disability and death. Elevated ApoB is one of these major risks.
What I am Doing to Reduce Cardiovascular Risks
If we could travel back in time to our youth and avoid secondhand smoke and atherogenic foods, exercise more, avoid early-life weight gain, maintain lower blood pressure, and take corrective actions where needed, atherosclerotic diseases would likely be a rarity.24
I envy younger people who have a lower rate of exposure to artery-damaging tobacco smoke. For many however, poor dietary habits and lack of corrective interventions will likely doom them to atherosclerotic risks that people over 65 face today (90% of men).25
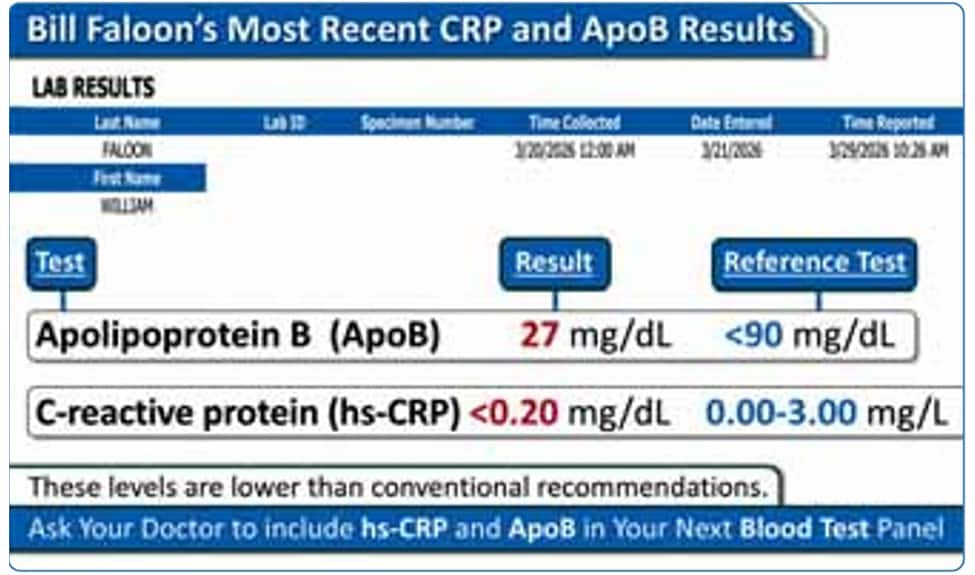
The chart below is consistent with what I achieved over the past several years as it relates to suppressing ApoB (and CRP).
Whether you target these very low ApoB numbers is a personal choice. However, a growing body of expert guidance, including the 2024 National Lipid Association Expert Clinical Consensus, is aiming for ApoB below 90 mg/dL in adults with borderline to intermediate risk. This lower level is associated with lower cardiovascular risk and has not been linked to adverse effects.14
Neutralize Harsh Realities with Comprehensive Blood Tests

Normal aging often results in dyslipidemia, which is the abnormal levels of artery-damaging lipids, including apolipoprotein B (ApoB).24
This contributes to the surge of ischemic stroke and heart disease older people confront.24,26
Early comprehensive blood testing reveals an opportunity to take corrective actions before a major medical event strikes.27,28
Many of the nutrients you already take, along with healthy dietary choices, have significant cardiovascular protecting properties.
But if a blood test result detects even a single risk factor, interventions using conventional and/or complementary approaches are highly recommended.
The graphic below my signature is used in my live presentations urging people not to think that avoiding a diagnostic or treatment will enable their problem to disappear.
You can view our Male and Female Blood Test Panels available at annual super sale pricing on the next page.
For longer life,
William Faloon, Co-Founder, Life Extension®
References
- Jovin DG, Sumpio BE, Greif DM. Manifestations of human atherosclerosis across vascular beds. JVS Vasc Insights. 2024 2024/01/01/;2:100089.
- Nedkoff L, Briffa T, Zemedikun D, et al. Global Trends in Atherosclerotic Cardiovascular Disease. Clinical Therapeutics. 2023 2023/11/01/;45(11):1087-91.
- Wang FM, Rozanski A, Arnson Y, et al. Cardiovascular and All-Cause Mortality Risk by Coronary Artery Calcium Scores and Percentiles Among Older Adult Males and Females. Am J Med. 2021 Mar;134(3):341-50 e1.
- Ceasovschih A, Banjanin N, Bednarek A, et al. Atherosclerotic features in patients with heart failure. Arch Med Sci. 2025;21(4):1107-29.
- Available at: https://aspe.hhs.gov/reports/cvd-report-congress. Accessed April 10, 2026.
- Available at: https://www.heart.org/en/health-topics/heart-failure/causes-and-risks-for-heart-failure. Accessed April 12, 2026.
- Baron DK, Weberndorfer V, Crijns H, et al. Association between atherosclerosis and atrial fibrillation progression in patients with paroxysmal atrial fibrillation: Data from the RACE V study. Am Heart J. 2026 Jun;296:107366.
- Pokorney SD, Berchuck SI, Chiswell K, et al. Atrial branch coronary artery stenosis as a mechanism for atrial fibrillation. Heart Rhythm. 2022 Aug;19(8):1237-44.
- Fleg JL, Forman DE, Berra K, et al. Secondary prevention of atherosclerotic cardiovascular disease in older adults: a scientific statement from the American Heart Association. Circulation. 2013 Nov 26;128(22):2422-46.
- Nasir K, Cainzos-Achirica M, Valero-Elizondo J, et al. Coronary Atherosclerosis in an Asymptomatic U.S. Population: Miami Heart Study at Baptist Health South Florida. JACC Cardiovasc Imaging. 2022 Sep;15(9):1604-18.
- Raitakari O, Pahkala K, Magnussen CG. Prevention of atherosclerosis from childhood. Nat Rev Cardiol. 2022 Aug;19(8):543-54.
- Blumenthal RS, Morris PB, Gaudino M, et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2026 Mar 13;0(0).
- Available at: https://www.lifeextension.com/magazine/2019/6/as-we-see-it. Accessed April 3, 2026.
- Soffer DE, Marston NA, Maki KC, et al. Role of apolipoprotein B in the clinical management of cardiovascular risk in adults: An Expert Clinical Consensus from the National Lipid Association. J Clin Lipidol. 2024 Sep-Oct;18(5):e647-e63.
- Boren J, Packard CJ, Binder CJ. Apolipoprotein B-containing lipoproteins in atherogenesis. Nat Rev Cardiol. 2025 Jun;22(6):399-413.
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N Engl J Med. 2017 May 4;376(18):1713-22.
- Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N Engl J Med. 2018 Nov 29;379(22):2097-107.
- Sniderman AD, Islam S, McQueen M, et al. Age and Cardiovascular Risk Attributable to Apolipoprotein B, Low-Density Lipoprotein Cholesterol or Non-High-Density Lipoprotein Cholesterol. J Am Heart Assoc. 2016 Oct 13;5(10).
- Ference BA, Graham I, Tokgozoglu L, et al. Reprint of: Impact of Lipids on Cardiovascular Health: JACC Health Promotion Series. J Am Coll Cardiol. 2018 Dec 11;72(23 Pt B):2980-95.
- Slipczuk L, Blankstein R, Bucciarelli-Ducci C, et al. State of the Art: Evaluation and Medical Management of Nonobstructive Coronary Artery Disease in Patients With Chest Pain: A Scientific Statement From the American Heart Association. Circulation. 2025 Dec 9;152(23):e443-e66.
- Machanahalli Balakrishna A, Kaushik S, Tandalam Palanivelu S, et al. Safety and Efficacy of Achieving Very Low LDL Cholesterol Concentrations with PCSK9 Inhibitors. J Clin Med. 2025 Jun 27;14(13).
- Bayturan O, Kapadia S, Nicholls SJ, et al. Clinical predictors of plaque progression despite very low levels of low-density lipoprotein cholesterol. J Am Coll Cardiol. 2010 Jun 15;55(24):2736-42.
- Nicholls SJ, Puri R, Anderson T, et al. Effect of Evolocumab on Progression of Coronary Disease in Statin-Treated Patients: The GLAGOV Randomized Clinical Trial. JAMA. 2016 Dec 13;316(22):2373-84.
- Pietri P, Stefanadis C. Cardiovascular Aging and Longevity: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021 Jan 19;77(2):189-204.
- Faridi KF, Malik D, Essa M, et al. 10-Year and 30-Year Risks of Cardiovascular Disease in the U.S. Population. J Am Coll Cardiol. 2025 Jun 17;85(23):2239-49.
- Goldstein LB, Adams R, Alberts MJ, et al. Primary Prevention of Ischemic Stroke. Stroke. 2006 2006/06/01;37(6):1583-633.
- Ridker PM, Moorthy MV, Cook NR, et al. Inflammation, Cholesterol, Lipoprotein(a), and 30-Year Cardiovascular Outcomes in Women. N Engl J Med. 2024 Dec 5;391(22):2087-97.
- White-Al Habeeb NMA, Higgins V, Wolska A, et al. The Present and Future of Lipid Testing in Cardiovascular Risk Assessment. Clin Chem. 2023 Apr 28;69(5):456-69.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun