Life Extension Magazine®
HOMOCYSTEINE AND HEART ATTACKS |
How SuperNutrients Can Protect YouBy Paul Frankel, Ph.D. and Terri Mitchell
Heart disease is the No. 1 killer in the U.S., killing more people than cancer, infectious diseases, and homocides combined. Nearly a third of all victims will not survive their first symptom. Half of all victims won't reach the hospital alive. For the past few decades, cholesterol has been the demon of heart disease. Fat consciousness has become America's favorite dietary preoccupation, with entire industries growing up around the idea of reducing dietary fat and cholesterol. While cholesterol is associated with heart disease in some studies, and Americans do eat too much fat, it appears that cholesterol may have less to do with heart disease than most people think. A much stronger case has emerged for a toxic amino acid called homocysteine. Homocysteine is a naturally synthesized by-product of methionine metabolism. If the right cofactors are present, it will eventually convert to cysteine and other beneficial compounds. If the cofactors are lacking, it will build up to toxic levels. Data from a study on healthy U.S. physicians with no prior history of heart disease shows that highly elevated homocysteine levels are associated with a more than three-fold increase in the risk of heart attack over a five-year period. This finding was published in 1992 in JAMA as part of the Physicians' Health Study. The study included 14,916 male physicians; it is the same one that showed the benefits of aspirin. The Framingham Heart Study and other studies have confirmed that elevated homocysteine is an independent risk factor for heart disease. It is especially imperative for people with a family history of cardiovascular disease to control their homocysteine levels. In one study, 37 men and women with early familial heart disease had 29% higher levels of homocysteine than controls. Dr. Rene Malinow of the Oregon Health Sciences Center concluded that some cases of elevated homocysteine could be the result of an inherited abnormality. This would be one explanation for premature coronary artery disease that runs in families. Mostly, however, elevated homocysteine levels can be traced to inadequate or improper nutrition. The Different Forms Of Heart DiseaseCardiovascular disease manifests as peripheral artery disease, coronary artery disease, myocardial infarction (heart attack), stroke, aneurysm, thromboembolism, extracranial carotid artery and stenosis. As an artery (or vein) becomes diseased, the inner arterial wall becomes thick - a condition known as arteriosclerosis. Cells lining the artery proliferate and combine with protein and lipids in a mass called an atherosclerotic plaque. Plaques are commonly the first indication of cardiovascular disease. Plaques change with time, gathering cholesterol and fat, finally becoming atheromas. Atheromas distort the artery wall, allowing calcification. Eventually, the inside of arteries become so rough that if you run your fingers over them, they feel like bits of broken glass. When an atheroma blocks blood to the heart, it is referred to as a heart attack. When it blocks blood to the brain, it is a stroke. If the penile artery is damaged or occluded, impotence results. Partial blockage in the chest (which causes pain) is referred to as angina, and weaknesses or rupturing of the arteries or veins are referred to as aneurysms. Homocysteine is thought to initiate these events by irritating the inner lining of arteries and veins. In addition, it was recently reported in the journal Circulation that hyperhomocysteinemia (high homocysteine) impairs blood vessels' ability to dilate, or expand. Millions of dollars are spent annually on drugs designed to lower blood pressure by dilating blood vessels. It is likely that in some people, this life-threatening problem could be reversed by the supernutrients that lower homocysteine. Stroke and HomocysteineAccording to a study in the European Journal of Clinical Investigation, 40% of stroke victims have elevated homocysteine compared to only 6% of controls. The study found increased homocysteine in lacunar, hemorrhagic and embolic strokes. A study published in Lancet in 1996 showed that even after adjustment for other risk factors, homocysteine was an independent risk factor for stroke and arterial thrombosis in patients with the autoimmune disease lupus. Another study published in Lancet came to the same conclusion after studying 107 middle-aged British men who participated in a 2-year investigation. The authors concluded that "these findings suggest that homocysteine is a strong and independent risk factor for stroke." It has even been reported that the level of homocysteine in blood correlates with the thickness of arteries. And it was reported in the Journal of Nutrition that men with levels of homocysteine above 14 µmol/L had a greater than 50% chance of stenosis in an extracranial carotid artery, whereas men with levels below 9.1 µmol/L only had a 27% incidence of stenosis. (The data for women were slightly different. Women with levels of homocysteine greater than 14.3 µmol/L had a 39% chance of having carotid artery stenosis: below 9.1 µmol/L, their chances were about even with men). A New Demon EmergesIn 1982, Edward Gruber and Stephen Raymond of MIT wrote in their book, Beyond Cholesterol: B6, Arteriosclerosis and Your Heart: "Homocysteine rapidly induces the initial states of arteriosclerosis and cholesterol's effects are not apparent." A comparison of the data on homocysteine with the data on cholesterol illustrates the strength of the homocysteine theory. There are many problems with the theory that dietary cholesterol causes heart disease. For one thing, non-oxidized cholesterol is not atherogenic in animals. Further, dietary cholesterol doesn't cause vascular disease in animals except under extreme conditions. Heart and vascular disease can be observed in the complete absence of added dietary cholesterol in animals. The cholesterol hypothesis preaches that a multitude of things increase the risk of heart attack. The list includes triglycerides, lipoprotein(a), fibrinogen, smoking, blood pressure, inactivity and poor genetics. Such a multiple risk factor approach should raise a red flag. Dr. Lewis Thomas (former president of Memorial Sloan-Kettering Cancer Center) has stated that every disease turns out to have one central mechanism of action. Cholesterol has too many ifs, ands and buts to be the cause of heart disease. Levels of cholesterol in blood do correlate with heart disease. However, cholesterol is no longer thought to be the cause of heart disease. Also, a recent study by Dr. Franziska Loehrer and co-workers at University Hospital in Switzerland showed that cholesterol and triglycerides failed to demonstrate a statistically significant correlation with coronary artery disease. Elevated homocysteine, low S-adenosylmethionine (SAM), age, and body mass index did. According to Dr. Loehrer: "...high levels of homocysteine occur before the disease. The finding of similar homocysteine values in patients after an interval (of approximately) one year supports the idea that this parameter [homocysteine] plays a role in the disease process and is not just altered by the disease itself." Homocysteine is a clearly-established risk factor for heart disease. Based on large and small-scale studies, it is a better predictor of heart attacks than cholesterol.
|
Known for Over Two Decades | |
How SuperNutrients Can Protect YouBy Paul Frankel, Ph.D. and Terri Mitchell None of this suprises Dr. Kilmer McCully. In 1969, while doing research at Harvard, McCully noticed that children with elevated levels of homocysteine (in a genetic condition known as homocystinuria) showed vascular degeneration similar to that which occurs in middle-aged people with heart disease. Children with homocystinuria often die of thromboembolism. Because this condition causes high levels of homocysteine to build up, McCully theorized that homocysteine might be a causal factor in heart disease. He then proceeded to prove that his theory was, in fact, correct.His work was not met with applause in the scientific community, which coalesced in a herd mentality around the concept of cholesterol. McCully was denied tenure, and soon left Harvard. In 1995, Meir Stampfer of Harvard recalled for NBC's Tom Brokaw what McCully went through for daring a different idea. Now, almost 30 years after he made his discovery, the scientific community has finally acknowledged that homocysteine is a strong predictor of heart disease. Today, McCully is continuing his homocysteine research at the Veteran's Administration Hospital in Providence, Rhode Island. His long-standing theory has finally been confirmed and accepted by the medical community.
|
The Word is Out on Homocysteine | |||
| By Paul Frankel, Ph.D. and Terri Mitchell The importance of homocysteine in relation to heart disease is becoming well-known outside of research institutes. In addition to NBC Nightly News with Tom Brokaw, articles have been published in Newsweek (2/17/97), The Wall Street Journal (8/19/92 and 2/2/95), The Los Angeles Times (7/4/96), Prevention magazine (7/94), and more. Spots have been aired on the radio by Cedars-Sinai Medical Center, and McCully is coming out with a new book. The relationship between homocysteine and heart disease is so firm that some insurance companies are paying for homocysteine testing in some circumstances. From JAMA to Prevention magazine, homocysteine has become the word in heart disease. An International Symposium is HeldIn 1995, the Journal of Nutrition (the official publication of the American Institute of Nutrition) asked researchers from around the world to present data on the relationship between homocysteine and heart disease.Dr. Peter Harpel of Mt. Sinai School of Medicine reported that lipoprotein(a) and fibrinogen damage the cardiovascular system much more actively in the presence of homocysteine. In the Hordaland Homocysteine Study of over 10,000 people in Norway, it was found that being female and taking vitamins were associated with low homocysteine levels. After reviewing the data, Dr. Lars Brattström of Kalmer County Hospital in Sweden reported that levels of homocysteine directly correlate with cardiovascular disease. A major theme of the seminar was that while some people may not respond to a particular homocysteine-lowering supplement, the combination of TMG, vitamin B6, folic acid, and vitamin B12 decreased homocysteine in nearly every patient. That's why the standard treatment for lowering homocysteine, from Prince Henry Hospital in Australia, to University Hospital Nijmegen in the Netherlands-to Harvard Medical School-is a supernutrient combination of TMG, B6, B12 and folic acid. Lowering HomocysteineSupernutrient dietary supplements, taken in the right amounts, can lower levels to normal in 95% of cases. Lowering homocysteine through supplements is the single most important and well-documented use of vitamins and quasi-vitamins to date. According to Dr. Stampfer of Harvard (and seven other researchers from well-known U.S. research institutions), Betaine (TMG or trimethylglycine), folic acid (folate), vitamin B12, vitamin B6, and choline are effective in lowering homocysteine.Unfortunately, neither researchers nor clinicians agree on what constitutes a safe level of homocysteine. One study has suggested that every 4µmol/L (4µmol/mL) increase in homocysteine equals a 40% increase in risk. Other studies confirm that there is a very fine line between what is a safe level and what is not. In the Physicians' Health Study, the men who had heart attacks or died of cardiovascular disease were separated in their homocysteine levels from the ones who didn't by only a few micromoles difference in homocysteine. It is far from clear at this point that any of the large-scale studies have been conducted long enough, and with sufficient scrutiny, to determine what is a safe level of homocysteine. There is no magic "cut-off" or "safe" level of homocysteine at the present time.Part of the problem may lie in the methods used to measure homocysteine. According to McCully's work, there are different forms of homocysteine - some of them more reactive than others. Presently, all homocysteine is measured together, without separating out the more damaging form. The situation is analogous to the problem with cholesterol: while it is oxidized cholesterol that is problematic, standard tests measure all cholesterol, and don't distinguish between oxidized and non-oxidized. The failure of both cholesterol and homocysteine tests to quantify the more dangerous forms of both substances causes problems when trying to determine what is safe and what is not safe. However, it does not negate the fact that both are associated with heart disease. People who are wondering whether they should have their homocysteine levels tested should be aware that certain risk factors are associated with elevated homocysteine. According to the Hordaland Homocysteine Study, being male, smoking cigarettes, and being over 65 raises the risk both for high homocysteine and heart attack. Elevated heart rate and blood pressure also are associated with elevated homocysteine. It also appears that lack of exercise and high cholesterol levels are particularly risky for men and women in their 40s. People who have one or more of these risk factors should be tested for their homocysteine levels. Laboratory reference ranges are not definitive, but they can give an indication of risk on the high end. There was a 3.4 increased risk of heart attack in the Physicians' Health Study when homocysteine levels were greater than 15.8 µmol/mL. Normally, homocysteine is a short-lived product in the body. There is no known danger in having too little of it.
Interestingly, most of the same supplements that lower homocysteine, elevate S-adenosylmethionine (SAM). SAM is a bioactive form of methionine that is made naturally in the body. It is what is known as a "methyl donor" because it contributes a methyl group (CH3) to other molecules to change their activity. SAM, as discussed in previous articles in Life Extension magazine, is critical for human health. The synthesized version has proven to be valuable therapy for several conditions, including liver cirrhosis, depression, osteoarthritis and fibromyalgia.
|
Vitamin B6 And Homocysteine | ||||||||
| By Paul Frankel, Ph.D. and Terri Mitchell Homocysteine's relationship to heart disease may explain some things that cholesterol never could. It may even explain the increase in heart disease which has occurred in women over the last two decades. Vitamin B6 helps the body lower levels of homocysteine. A rise in heart disease in women coincides with the use of birth control pills. Birth control pills deplete vitamin B6 and raise levels of homocysteine.
Smoking is a known risk factor for heart disease. Coincidentally, cigarette smoke also depletes Vitamin B6. Low B6 has been shown to correlate with high levels of homocysteine. Researchers in Norway recently found that a combination of smoking and drinking coffee is a sure ticket to elevated homocysteine. It's not surprising that the statistics linking smoking to heart disease are similar to those linking high homocysteine levels to heart disease.
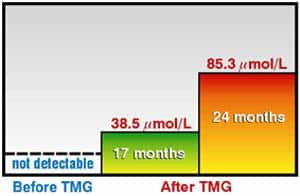
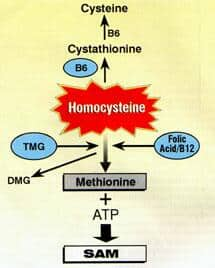
Supernutrients Versus GenesThe remarkable potency of the supernutrient combination (TMG, B6, B12, folic acid and choline) can be seen in people with genetic defects in enzyme production that cause elevated homocysteine. People with these disorders frequently die of cardiovascular disease. A striking case was reported by Dr. T. Kishi and his group in the Journal of Inherited Metabolic Diseases. The authors reported that a 16 year-old Japanese girl had no detectable SAM in her body. She was unable to walk, with or without support, and had severe peripheral neuropathy, muscle weakness and convulsions. Her vascular system was on the verge of collapse. Therapy with vitamins B6 or B12 didn't work. Folate (folic acid) lowered homocysteine, but didn't improve the young woman's symptoms. But two months after adding trimethylglycine (TMG or betaine) to the regimen, her homocysteine level dropped, and she improved and was able to walk with support. Seventeen months later, she was free from convulsions and able to walk normally again.This case history demonstrates the see-saw relationship between homocysteine and SAM. The young woman's SAM levels went from undetectable to near normal after the first few months of treatment, while her homocysteine levels - which started out too high - fell dramatically. The see-saw relationship between "good" SAM and "bad" homocysteine is very evident in this case. If these nutrients can overcome a genetic disorder, consider how powerful they can be in reducing the risks associated with elevated homocysteine in the general population. The Biochemistry of HomocysteineThere are three biochemical pathways used by the body to reduce homocysteine. In one pathway, TMG donates a methyl group which detoxifies homocysteine. In this reaction, TMG is turned into dimethylglycine (DMG) - yes, that familiar product sold as a supplement for its energizing effects. In the other routes, folic acid, B12 and B6 convert homocysteine into non-toxic substances. Some people can't utilize one or another of these pathways. That is why a combination of all the supernutrients is the only way to guarantee that homocysteine will be lowered. Nearly all cases of elevated homocysteine can be corrected with a combination of TMG, folic acid, vitamin B12, and vitamin B6. A note about vitamin B6 (pyridoxine): B6 can be toxic in high doses. Some people who take more than 250 mg/day have developed tingling and numbness in their hands and feet, and balance problems. If you develop any of these problems, consult your doctor immediately. The symptoms of vitamin B6 toxicity will subside when the dose of the vitamin is reduced. People taking levodopa (L-dopa) should consult their doctor before taking supernutrients. Homocysteine and DietDr. Soo-Sang Kang of Rush Medical College in Chicago, reports that, along with genetic predisposition, elevated levels of homocysteine occur because of nutritional inadequacies. B6, B12 and folate deficiencies are common in people of all ages. Betaine deficiency has not yet been studied in the general population. Although vitamin B6 is found in a variety of foods, processing, canning, and freezing quickly destroy it. Folic acid (originally found in spinach) is in most leafy vegetables, yet numerous studies indicate that people of all ages and cultures are deficient. In one study of healthy elderly patients, one or more elevated metabolites (indicating deficiency) were found in 63% of people tested. Using the metabolite method of measuring these vitamins reveals even greater deficiencies than suspected. In elderly hospitalized patients, 83% showed a deficiency in folic acid. In another study on elderly Spanish people, low folate levels correlated with an impaired mental state and diminished ability to carry out daily activities. The Nationwide Food Consumption Survey of 1980 showed that half of all Americans surveyed were getting less than the RDA of vitamin B6. Vitamin B12 is found in anything that moves, but is reduced by antibiotics (which are used in most commercial animal farms). TMG (betaine) is found in most vegetables, and small fish and shrimp, although it requires great effort to get enough TMG through the diet to consistently lower homocysteine levels. Coffee may act as a inhibitor of betaine metabolism. A quick look at the standard Western diet (where the french fry has made the potato the most commonly eaten vegetable) reveals the roots of heart disease. Homocysteine is a product of methionine, an amino acid found in meat protein. It promotes heart disease by promoting the oxidation of lipids. Homocysteine plays a role in the entire heart disease process. It causes platelets to stick together; enhances the binding of Lp(a) to fibrin; and promotes free radical damage to the inside of arteries. Autopsies of young men killed in Vietnam show that vascular degeneration begins very early in Western society - likely due to the American high protein/fat diet which is deficient in supernutrient-containing vegetables.
A Long-Term StudyDr. Nicholas Dudman and his group of the University of New South Wales studied 10 people with homocystinuria (genetically-elevated homocysteine levels) who took TMG plus supernutrients vitamin B6 and folic acid for almost 13 years. They found that the TMG supernutrient combination kept homocysteine levels to one-fourth their pre-TMG level, with no negative side effects. According to the researchers, "it was necessary to continue taking TMG (betaine) regularly to maintain maximum effects." Homocysteine levels would rise within days if people neglected to take the combination; but quickly decreased once the TMG was resumed. The study is particularly striking in that homocysteine levels naturally rise with age, but in the patients taking TMG, levels actually fell substantially, even though the participants were getting older. |

Personal Reports on Long-Term Use |
| By Paul Frankel, Ph.D. and Terri Mitchell Some people have been taking homocysteine-lowering supernutrients for more than a decade. They have reported many benefits, including fewer colds, more energy, increased endurance, and lower blood sugar levels. Whether these effects are due to a decrease in homocysteine, an increase in SAM, or simply coincidence is not yet known. Blood sugar balance may relate to the osmotic protective feature of TMG. (The reason sugar beets contain so much TMG is to protect them against the stress sugar puts on plant cells). The Future of Homocysteine ResearchHomocysteine levels rise as people age. Therefore, any anti-aging program must take homocysteine levels into consideration. Lowering homocysteine has benefits beyond heart protection. It also protects against strokes. And the same supernutrients that lower homocysteine elevate SAM. SAM has numerous health benefits. Some important research on HIV-positive patients and homocysteine may prove beneficial for everyone. Dr. Müller and his co-workers at the University of Bergen in Norway report in the American Journal of Clinical Nutrition that AIDS patients have elevated concentrations of a particularly reactive form of homocysteine. This is thought to be related to the formation of reactive oxygen species caused by poor methylation. If this proves to be true, it may turn out that there is a relationship between homocysteine, free radicals and immunity. AIDS dementia has been correlated with low SAM levels. Dementia is something that usually occurs with advancing age. The research being done on AIDS dementia may give insight into the age-related version. A Major Breakthrough in Cardiovascular HealthWhile the potential benefits of lowering homocysteine and elevating SAM are just beginning to be realized, it is clear that there is a strong connection between homocysteine, heart disease, and stroke. With new blood tests for monitoring homocysteine, supernutrient supplementation, a proper diet and lifestyle plan (such as Dr. Ornish's program), there is no doubt that the incidence of heart disease will decline. Prevention is key. Don't wait until a heart condition strikes you down. The simple measures discussed in this article, combined with adequate blood monitoring, can help ensure that you don't fall victim to heart disease. How To Take Homocysteine-Lowering NutrientsFor the best results, a combination of homocysteine-lowering nutrients should be taken. TMG (betaine), Folic acid (folate), vitamin B6 (pyridoxine) and vitamin B12 are the nutrients which have been found to lower homocysteine in clinical studies. They all contribute something along the biochemical pathways which break down homocysteine. While any one of these factors by itself may lower homocysteine in some people, the best insurance is to take all of them. The methionine pathway is like a giant feedback loop with rest stops along the way. At those rest stops, nutrient co-factors are "fed" to the chemical reaction to keep it going. If any of these co-factors is not available, a toxic build-up of natural chemicals can result, and the entire pathway can become blocked. Based on the latest-available research from the lab of Dr. Craig Cooney, the basic homocysteine-lowering formula per day is: 1000 mg of TMG, 800 mcg folic acid, 500 mcg vitamin B12, and 50 mg vitamin B6. People with serious medical conditions can take up to 6 grams of TMG per day. No toxicity has been reported at this amount. TMG is a natural substance found abundantly in sugar beets. Homocysteine level should be monitored, and TMG dose adjusted accordingly. Vitamin B6 can be toxic in high doses. Problems have been reported at doses above 250 mg/day. Tingling, numbness and balance problems are signs of B6 toxicity. People taking L-dopa should not take supernutrients without first consulting with their physician.
|
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun