Life Extension Magazine®
The potential to heal once incurable degenerative diseases such as cancer or heart disease by regenerating cells that have failed or are about to fail is now within our grasp, thanks to the emergence of an exciting new field of medicine: regenerative medicine using adult stem cells. Indeed, tissues such as heart muscle that were long thought to be non-renewable have now been shown to be regenerated through this novel therapy. By using adult stem cells, scientists have avoided the controversy that has stymied advanced embryonic stem cell research in the past. Adult stem cell therapy offers an unprecedented step forward in the history of medicine and the applications of this new form of regenerative medicine are potentially unlimited. Embryonic versus Adult Stem CellsConsiderable confusion surrounds the use of stem cells, not only with the general public, but indeed with scientists and physicians. This confusion has been compounded by the ethical, moral, and political issues that have arisen around the sources of stem cells. Broadly speaking, there are two classifications of stem cells: those that are derived from embryos (embryonic stem cells, ESCs) and those that come from other sources (adult stem cells [ASCs] or somatic stem cells). All stem cells, whatever their source, have three general properties: they are capable of dividing and renewing themselves for long periods; they are undifferentiated; and they have the ability to develop into specialized cell types. Embryonic stem cells are derived from a clump of cells formed after fertilization, which is called the inner cell mass (ICM). The cells of the ICM rapidly differentiate to form all of the cell types in the human body, hence creating a fetus and then a human being. If the cells of the ICM are harvested and grown in appropriate culture conditions, however, they will replicate indefinitely and, when suitably stimulated, will differentiate into three germ layers: ectoderm, mesoderm, and endoderm—representing any cell lineage of the body. This potential to differentiate into any other cell type in the body is referred to as plasticity (or pluripotency).1 Given their high degree of plasticity, however, embryonic stem cells not only have the capability of becoming beneficial tissue, they also can differentiate into cancerous (malignant) cells. While it has recently been reported that these cells can be derived from sources other than embryos, there is broad consensus that much more research is required before human therapies based on embryonic stem cells can be safely pursued.2 Thus, while these cells have great importance in unraveling the processes by which cells proliferate and differentiate, there are currently no approved treatments or human trials using embryonic stem cells. In contrast, adult stem cells are derived from non-embryonic origins, including bone marrow, peripheral blood and, paradoxically, cord blood, placental cells, and amniotic fluid (note that cord blood and placental cells must be collected and banked at the time of birth for future use, while amniotic fluid is drawn from the fluid surrounding a growing fetus). Adult stem cells are thought to be capable of facilitating all the body’s natural repair processes. Since the production of adult stem cells does not require the destruction of an embryo, these cells are not associated with any ethical or political controversy. Readily obtainable, these cells have been used for many years for therapeutic purposes.
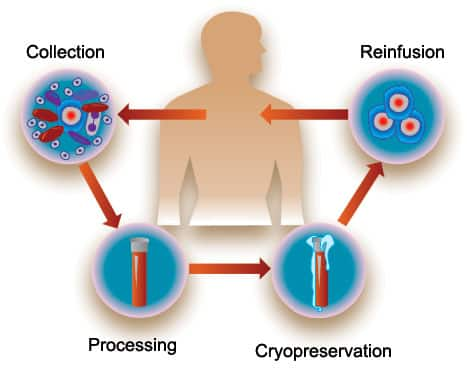
Adult Stem Cell TherapiesIt was initially believed that the ability of adult stem cells to regenerate tissue was limited to the type of tissue in which they resided. This is now known not to be the case. Numerous studies have confirmed that, although these cells do not have the universality of the embryonic type, they do have the capacity for self-renewal, are able to differentiate into other cell types and are capable of generating differentiated cell progenitors (similar to stem cells) of different (perhaps all) cell lineages. Their potential to differentiate into cell types found in other tissues means they can travel to a site of damage, penetrate the damaged tissue, and then regenerate this tissue by a process called transdifferentiation. It is these properties that have formed the basis for therapies in which adult stem cells have been used. Bone Marrow Transplants: Adjuvant Cancer CareOne of the areas in which adult stem cells have become widely used is in the treatment of blood cancers including leukemia, lymphoma, and multiple myeloma. Since the 1990s, bone marrow transplants using blood-derived stem cells, which are capable of generating all cell types of the blood and immune system, have been used to regenerate bone marrow damaged by the effects of chemotherapy and/or radiation. Without healthy bone marrow, patients with these cancers cannot make the blood cells needed to carry oxygen, fight infection, and heal wounds. Healthy, transplanted bone marrow therefore restores these functions. Stem Cell DonorsOften, because of the lack of an identical donor, adult stem cells obtained from a genetically well-matched healthy donor are infused into the affected recipient (known as “allogeneic” infusion, as opposed to using a recipient’s own stem cells) to create a healthy immune system free of cancer. These donor stem cells are obtained by a technique called apheresis, in which a machine selectively separates stem cells from donor blood and returns the rest of the blood to the donor. During this process, the donor most often receives a medicine (or “mobilizing agent”) called granulocyte colony-stimulating factor, which stimulates the bone marrow to release stem cells into the bloodstream where they can be easily collected after several days of treatment. Although this method has proved successful in providing sustained remission or cures of underlying diseases, donor stem cells do pose problems in that they can either be rejected by the recipient’s immune system or they may attack the recipient’s cells in a serious condition called graft-versus-host disease. In order to reduce the magnitude of rejection and graft-versus-host disease, tissue from both the donor and recipient must be matched to be as compatible as possible. Often, recipients must take immunosuppressive drugs for the rest of their lives to prevent rejection, which is associated with morbidities such as increased risk of serious infections.3,4 An alternative to using closely matched donor stem cells (“allogeneic” infusion) is to use the recipient’s own stem cells, known as “autologous” infusion. The use of these “autologous” cells avoids all of the problems associated with donor stem cells and also confers significant clinical and economic benefits. Intuitively, collecting and banking blood-derived stem cells many years before the onset of disease, known as pre-disease harvesting, should minimize the presence of tumor cells or tumor stem cells. Furthermore, banking an individual’s own stem cells may one day be life-saving in the event—particularly in those with strong family or occupational related risk factors for cancer—that a diseased organ needs to be replaced with one grown from their own cells.
Restoring Heart FunctionHeart disease shows some of the greatest potential for the application of stem cells. Ischemic heart disease accounts for approximately half of all cardiovascular deaths in the United States, with over one million people suffering a heart attack each year. A heart attack leads to the death of the heart tissue and causes the muscle cells of the heart to be depleted. It also progressively remodels the structure of the heart, further reducing its ability to pump blood. For a long time, it was believed that the heart was a “post-mitotic” (non-renewable) organ composed of muscle cells that had completed the differentiation process, and therefore had limited capability of regeneration following an injury such as a heart attack. This belief is now being effectively challenged by mounting evidence to show that not only do endogenous self-repairing mechanisms exist, but that these and other regenerative processes, such as the development of new blood vessels, can be activated, or facilitated, by adult stem cells. These findings, and other observations, have led to a number of clinical trials that have tested the ability of stem cells to restore heart function in patients with acute heart disease. Early studies focused on establishing the safety and feasibility of using a patient’s own stem cells to improve heart function following a heart attack.5-7 Although research is ongoing, many controlled studies have also compared similar groups of patients on standard medical therapy after a heart attack with those on therapy plus an intracoronary infusion of their own stem cells. The results have been encouraging, revealing a positive effect of stem cell therapy on improving cardiac function outcomes, such as blood flow within the heart, wall motion, left ventricular function, and reducing the size of damaged heart tissue.8-17
| |||||||||||



Better Long-Term Cardiac HealthAdult stem cell therapies have also shown clinical benefit in severe chronic heart disease, such as congestive heart failure, of which almost half a million new cases are diagnosed each year. In one study by Brehm and Strauer, bone marrow-derived stem cells were transplanted directly into the heart tissue of 18 male patients who had suffered a heart attack between five months and 8.5 years earlier.18 These patients had progressive chronic heart failure with reduced left ventricular function. A group of patients who did not receive any cell therapy served as controls. After three months, the researchers found that the area of heart tissue damaged by disease was reduced, while oxygen uptake, energy metabolism and left ventricular function all increased compared with the control group, who showed no significant changes in these parameters. In another study, Patel and colleagues studied 20 patients with severe chronic heart disease and very poor left ventricular function classified as chronic heart failure.19 All 20 patients received bypass surgery to improve blood flow. In addition, half of the patients also received an infusion of adult stem cells during surgery, which were injected into the most severely compromised regions of the heart. Six months after surgery, the left ventricular function of the stem cell-treated group increased substantially compared with the control group. The improvement was so great that the stem cell recipients were no longer defined as having chronic heart failure.
Banking Stem Cells for Heart HealthIt has been suggested that an alternative to stem cell infusion is to administer growth factors that are produced naturally in the body. The use of these chemicals, such as granulocyte colony-stimulating growth factor, alone stimulates the endogenous production of stem cells, which might obviate the need for stem cell infusion. However, a defined benefit from this therapy has not yet been established20 and some evidence suggests that the use of stem cells immediately after a heart attack may even be detrimental.21 Furthermore, there is mounting evidence that those factors that precipitate the onset of heart disease—such as hypertension, diabetes, smoking, and others—also impact the effectiveness of stem cells in terms of their ability to migrate, transdifferentiate, and proliferate. The benefits of banking stem cells before the onset of disease will undoubtedly prove to be clinically important as the use of these therapies becomes more widespread. Despite the uncertainties about their mechanisms of action, scientists broadly agree on the potential of regenerating damaged heart tissue using a patient’s own stem cells to improve cardiac function and performance.22 Autoimmune and Neurological ConditionsAdult stem cells could also offer hope for patients with autoimmune and neurodegenerative diseases.
In autoimmune disorders, the body begins to produce a type of white blood cells called T lymphocytes and protective proteins called antibodies, which, instead of protecting the body against invasive microbes and cancers, attack its own cells and organs. There are more than 70 different types of autoimmune disorders, for example, multiple sclerosis, rheumatoid arthritis, systemic sclerosis (scleroderma), systemic lupus erythematosus, and juvenile idiopathic arthritis. As a class, autoimmune diseases affect approximately 5% of the US population, with common conditions such as systemic lupus erythematosus affecting 1.5 million people, mostly young women. The standard treatment for autoimmune diseases generally consists of immunosuppression, anti-inflammatory medication, or anti-malarial medication, in addition to supportive care. In cases that do not respond to standard treatment or are considered life- or organ-threatening, high doses of immunosuppressive medication have been proposed as a treatment option to eliminate the T cells causing the autoimmune response. However, such high doses also suppress the bone marrow’s production of blood cells (known as “myelosuppression”), necessitating rescue therapy with transfused hematopoietic (blood cell-forming) stem cells.
It has been theorized that regenerating bone marrow with transplanted stem cells normalizes the immune system.23,24 The concept of stem cell therapy following immunosuppressive therapy for autoimmune diseases has led to the publication of consensus guidelines and the initiation of a number of well-controlled clinical trials.25,26 To date, more than 700 patients have received transplants using their own stem cells as treatment for severe autoimmune diseases,27 including 183 patients with multiple sclerosis,28 76 patients with severe rheumatoid arthritis,29 102 patients with systemic sclerosis (scleroderma),30,31 103 patients with systemic lupus erythematosus,32-34 and, most recently, 15 individuals with new onset type I diabetes.35 Numerous studies using adult stem cells to treat other autoimmune diseases such as Crohn’s disease, Behcet’s disease, and relapsing polychondritis have also been published.36,37 Early studies in patients with neurodegenerative diseases—some of which may represent autoimmune processes—have shown promising results, suggesting that stem cells might offer hope for people with neurological disorders, perhaps even for prevalent conditions such as Parkinson’s disease.38-41 Although the clinical outcomes of stem cell treatments have been variable, most of the studies in this field have shown significant amelioration of disease activity, improvement in serological (blood) markers, and either stabilization or reversal of organ dysfunction. The preliminary conclusions of these studies are sufficiently encouraging to proceed to randomized prospective trials of stem cell transplantation for autoimmune diseases as a group, and particularly for those that are most severe and debilitating. Similarly, scientists believe that stem cells therapies offer compelling hope for neurological conditions, and are further exploring their applications for these debilitating disorders.
Current and Future Stem Cell TherapiesImportantly, all of the studies that have been mentioned so far were carried out using stem cells that were collected after the onset of disease. It is intriguing to speculate on the improvement in outcome that might be achieved if a patient’s own stem cells were available before the onset of disease. The table on page 46 summarizes the current status of regenerative therapy, divided into those diseases being treated with adult stem cells today and those in which experimental evidence from animal studies strongly indicates potential benefits in the future.
ConclusionAdult stem cells may one day yield cures for the most dreaded diseases that plague adults. A plentiful supply of adult stem cells for personal use collected while healthy and available may offer all adults powerful insurance against the consequences of a range of diseases, both chronic and acute, that is growing daily. Only by having a readily accessible source of stem cells can the full benefits of regenerative medicine be realized. While it remains to be seen whether adult stem cells can prevent or reverse aging or extend life span, ongoing research promises to propel the field of regenerative medicine forward. Regardless of these unanswered questions, it is clear that banking stem cells for long-term storage may truly represent a “bio-insurance policy” that can help provide for your optimal health in the future. Authors’ AffiliationsDenis Rodgerson, PhD: NeoStem California Laboratory, 637 South Lucas Avenue, Suite 508, Los Angeles, CA 90017. Ron Rothenberg, MD, FACEP: California HealthSpan Institute, 320 Santa Fe Drive, Encinitas, CA 92024. Wayne Marasco, MD, PhD: Department of Cancer Immunology and AIDS, Dana-Farber Cancer Institute, Harvard Medical School, 44 Binney Street, Boston, MA 02115. Disclosures: All three authors have a financial interest in NeoStem, Inc. (www.neostem.com), a company that specializes in the banking and long-term storage of adult stem cells. If you have any questions about the scientific content of this article, please call one of our Health Advisors at 1-800-226-2370. | ||||||||||||||||||||||||||||||||||
| References | ||||||||||||||||||||||||||||||||||
| 1. Thomson JA, Itskovitz-Eldor J, Shapiro SS, et al. Embryonic stem cell lines derived from human blastocysts. Science. 1998 Nov 6;282(5391):1145-7. 2. Rossant J. Stem cells: the magic brew. Nature. 2007 Jul 19;448(7151):260-2. 3. Anon. Allogeneic peripheral blood stem-cell compared with bone marrow transplantation in the management of hematologic malignancies: an individual patient data meta-analysis of nine randomized trials. J Clin Oncol. 2005 Aug 1;23(22):5074-87. 4. Cutler C, Li S, Ho VT, et al. Extended follow-up of methotrexate-free immunosuppression using sirolimus and tacrolimus in related and unrelated donor peripheral blood stem cell transplantation. Blood. 2007 Apr 1;109(7):3108-14. 5. Kocher AA, Schuster MD, Szabolcs MJ, et al. Neovascularization of ischemic myocardium by human bone-marrow-derived angioblasts prevents cardiomyocyte apoptosis, reduces remodeling and improves cardiac function. Nat Med. 2001 Apr;7(4):430-6. 6. Fuchs S, Baffour R, Zhou YF, et al. Transendocardial delivery of autologous bone marrow enhances collateral perfusion and regional function in pigs with chronic experimental myocardial ischemia. J Am Coll Cardiol. 2001 May;37(6):1726-32. 7. Schuster MD, Kocher AA, Seki T, et al. Myocardial neovascularization by bone marrow angioblasts results in cardiomyocyte regeneration. Am J Physiol Heart Circ Physiol. 2004 Aug;287(2):H525-32. 8. Strauer BE, Brehm M, Zeus T, et al. Repair of infarcted myocardium by autologous intracoronary mononuclear bone marrow cell transplantation in humans. Circulation. 2002 Oct 8;106(15):1913-8. 9. Assmus B, Schachinger V, Teupe C, et al. Transplantation of Progenitor Cells and Regeneration Enhancement in Acute Myocardial Infarction (TOPCARE-AMI). Circulation. 2002 Dec 10;106(24):3009-17. 10. Britten MB, Abolmaali ND, Assmus B, et al. Infarct remodeling after intracoronary progenitor cell treatment in patients with acute myocardial infarction (TOPCARE-AMI): mechanistic insights from serial contrast-enhanced magnetic resonance imaging. Circulation. 2003 Nov 4;108(18):2212-8. 11. Schachinger V, Assmus B, Britten MB, et al. Transplantation of progenitor cells and regeneration enhancement in acute myocardial infarction: final one-year results of the TOPCARE-AMI Trial. J Am Coll Cardiol. 2004 Oct 19;44(8):1690-9. 12. Wollert KC, Meyer GP, Lotz J, et al. Intracoronary autologous bone-marrow cell transfer after myocardial infarction: the BOOST randomised controlled clinical trial. Lancet. 2004 Jul 10;364(9429):141-8. 13. Drexler H, Meyer GP, Wollert KC. Bone-marrow-derived cell transfer after ST-elevation myocardial infarction: lessons from the BOOST trial. Nat Clin Pract Cardiovasc Med. 2006 Mar;3 Suppl 1S65-8. 14. Schachinger V, Erbs S, Elsasser A, et al. Intracoronary bone marrow-derived progenitor cells in acute myocardial infarction. N Engl J Med. 2006 Sep 21;355(12):1210-21. 15. Assmus B, Honold J, Schachinger V, et al. Transcoronary transplantation of progenitor cells after myocardial infarction. N Engl J Med. 2006 Sep 21;355(12):1222-32. 16. Lunde K, Solheim S, Aakhus S, et al. Intracoronary injection of mononuclear bone marrow cells in acute myocardial infarction. N Engl J Med. 2006 Sep 21;355(12):1199-209. 17. Janssens S, Dubois C, Bogaert J, et al. Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevation myocardial infarction: double-blind, randomised controlled trial. Lancet. 2006 Jan 14;367(9505):113-21. 18. Brehm M, Strauer BE. Stem cell therapy in postinfarction chronic coronary heart disease. Nat Clin Pract Cardiovasc Med. 2006 Mar;3 Suppl 1S101-4. 19. Patel AN, Geffner L, Vina RF, et al. Surgical treatment for congestive heart failure with autologous adult stem cell transplantation: a prospective randomized study. J Thorac Cardiovasc Surg. 2005 Dec;130(6):1631-8. 20. Ince H, Petzsch M, Kleine HD, et al. Prevention of left ventricular remodeling with granulocyte colony-stimulating factor after acute myocardial infarction: final 1-year results of the Front-Integrated Revascularization and Stem Cell Liberation in Evolving Acute Myocardial Infarction by Granulocyte Colony-Stimulating Factor (FIRSTLINE-AMI) Trial. Circulation. 2005 Aug 30;112(9 Suppl):I73-80. 21. Kang HJ, Kim HS, Zhang SY, et al. Effects of intracoronary infusion of peripheral blood stem-cells mobilised with granulocyte-colony stimulating factor on left ventricular systolic function and restenosis after coronary stenting in myocardial infarction: the MAGIC cell randomised clinical trial. Lancet. 2004 Mar 6;363(9411):751-6. 22. Bartunek J, Dimmeler S, Drexler H, et al. The consensus of the task force of the European Society of Cardiology concerning the clinical investigation of the use of autologous adult stem cells for repair of the heart. Eur Heart J. 2006 Jun;27(11):1338-40. 23. Burt RK, Traynor AE. Hematopoietic stem cell transplantation: a new therapy for autoimmune disease. Stem Cells. 1999;17(6):366-72. 24. Gratwohl A. Passweg J. Gerber I. et al. Stem cell transplantation for autoimmune diseases. Best Pract Res Clin Haematology. 2001;14:755. 25. Tyndall A, Gratwohl A. Blood and marrow stem cell transplants in auto-immune disease: a consensus report written on behalf of the European League against Rheumatism (EULAR) and the European Group for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant. 1997 Apr;19(7):643-5. 26. Marmont A. Tyndall A. Gratwold A. Vischer T. Haemapoietic precursor-cell transplants for autoimmune disease. Lancet. 1995;345:978. 27. Tyndall A, Saccardi R. Haematopoietic stem cell transplantation in the treatment of severe autoimmune disease: results from phase I/II studies, prospective randomized trials and future directions. Clin Exp Immunol. 2005 Jul;141(1):1-9. 28. Saccardi R, Kozak T, Bocelli-Tyndall C, et al. Autologous stem cell transplantation for progressive multiple sclerosis: update of the European Group for Blood and Marrow Transplantation autoimmune diseases working party database. Mult Scler. 2006 Dec;12(6):814-23. 29. Snowden JA, Passweg J, Moore JJ, et al. Autologous hemopoietic stem cell transplantation in severe rheumatoid arthritis: a report from the EBMT and ABMTR. J Rheumatol. 2004 Mar;31(3):482-8. 30. Burt RK, Marmont A, Oyama Y, et al. Randomized controlled trials of autologous hematopoietic stem cell transplantation for autoimmune diseases: the evolution from myeloablative to lymphoablative transplant regimens. Arthritis Rheum. 2006 Dec;54(12):3750-60. 31. Loh Y, Oyama Y, Statkute L, et al. Non-myeloablative allogeneic hematopoietic stem cell transplantation for severe systemic sclerosis: graft-versus-autoimmunity without graft-versus-host disease? Bone Marrow Transplant. 2007 Apr;39(7):435-7. 32. Jayne D, Tyndall A. Autologous stem cell transplantation for systemic lupus erythematosus. Lupus. 2004;13(5):359-65. 33. Jayne D, Passweg J, Marmont A, et al. Autologous stem cell transplantation for systemic lupus erythematosus. Lupus. 2004;13(3):168-76. 34. Burt RK, Traynor A, Statkute L, et al. Nonmyeloablative hematopoietic stem cell transplantation for systemic lupus erythematosus. JAMA. 2006 Feb 1;295(5):527-35. 35. Voltarelli JC, Couri CE, Stracieri AB, et al. Autologous nonmyeloablative hematopoietic stem cell transplantation in newly diagnosed type 1 diabetes mellitus. JAMA. 2007 Apr 11;297(14):1568-76. 36. Hensel M, Breitbart A, Ho AD. Autologous hematopoietic stem-cell transplantation for Behcet’s disease with pulmonary involvement. N Engl J Med. 2001 Jan 4;344(1):69. 37. Hawkey CJ, Snowden JA, Lobo A, Beglinger C, Tyndall A. Stem cell transplantation for inflammatory bowel disease: practical and ethical issues. Gut. 2000 Jun;46(6):869-72. 38. Lindvall O, Kokaia Z, Martinez-Serrano A. Stem cell therapy for human neurodegenerative disorders-how to make it work. Nat Med. 2004 Jul;10: SupplS42-S50. 39. Dezawa M, Kanno H, Hoshino M, et al. Specific induction of neuronal cells from bone marrow stromal cells and application for autologous transplantation. J Clin Invest. 2004 Jun;113(12):1701-10. 40. Takagi Y, Takahashi J, Saiki H, et al. Dopaminergic neurons generated from monkey embryonic stem cells function in a Parkinson primate model. J Clin Invest. 2005 Jan;115(1):102-9. 41. Behrstock S, Ebert A, McHugh J, et al. Human neural progenitors deliver glial cell line-derived neurotrophic factor to parkinsonian rodents and aged primates. Gene Ther. 2006 Mar;13(5):379-88. 42. Ballen K, Broxmeyer HE, McCullough J et al. Current status of cord blood banking and transplantation in the United States and Europe. Biol Blood Marrow Transplant. 2001;7(12):635-45. 43. Bacigalupo A, Frassoni F, Van Lint MT. Bone marrow or peripheral blood as a source of stem cells for allogeneic transplants. Curr Opin Hematol. 2000 Nov;7(6):343-7. 44. Available at: www.marrow.org/ABOUT/index.html. Accessed July 11, 2007. 45. Rawley S. Cryopreservation of hematopoietic cells. In Thomas’ Hematopoietic Cell Transplantation. Eds.Blume K. Foreman S. Appelbaum F. Third Edition, P 599. Blackwell Publishing, Malden, MA 2004. 46. Bickford PC, Tan J, Shytle RD, et al. Nutraceuticals synergistically promote proliferation of human stem cells. Stem Cells Dev. 2006 Feb;15(1):118-23. 47. Shankar S, Singh G, Srivastava RK. Chemoprevention by resveratrol: molecular mechanisms and therapeutic potential. Front Biosci. 2007 Sep 1;12:4839-54. 48. Ingram DK, Zhu M, Mamczarz J, et al. Calorie restriction mimetics: an emerging research field. Aging Cell. 2006 Apr;5(2):97-108. 49. Chen JF, Huang L, Jin J, et al. Relationship between aging and the number and function of bone marrow-derived endothelial progenitor cells in rats. Zhonghua Xin Xue Guan Bing Za Zhi. 2006 Nov;34(11):1026-8. 50. J G, Cq W, Hh F, et al. Effects of resveratrol on endothelial progenitor cells and their contributions to reendothelialization in intima-injured rats. J Cardiovasc Pharmacol. 2006 May;47(5):711-21. 51. Kawakita E, Hashimoto M, Shido O. Docosahexaenoic acid promotes neurogenesis in vitro and in vivo. Neuroscience. 2006;139(3):991-7. 52. Kidd PM. Neurodegeneration from mitochondrial insufficiency: nutrients, stem cells, growth factors, and prospects for brain rebuilding using integrative management. Altern Med Rev. 2005 Dec;10(4):268-93. 53. Thum T, Hoeber S, Froese S, et al. Age-dependent impairment of endothelial progenitor cells is corrected by growth-hormone-mediated increase of insulin-like growth-factor-1. Circ Res. 2007 Feb 16;100(3):434-43. 54. Imanishi T, Hano T, Nishio I. Estrogen reduces endothelial progenitor cell senescence through augmentation of telomerase activity. J Hypertens. 2005 Sep;23(9):1699-706. 55. Liu KQ, Qi X, Du JP, et al. Treatment of acute myocardial infarction with autologous bone marrow stem cells mobilization combined with recombinant growth factor in rat. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2006 Aug;18(8):494-7. 56. Iwakura A, Shastry S, Luedemann C, et al. Estradiol enhances recovery after myocardial infarction by augmenting incorporation of bone marrow-derived endothelial progenitor cells into sites of ischemia-induced neovascularization via endothelial nitric oxide synthase-mediated activation of matrix metalloproteinase-9. Circulation. 2006 Mar 28;113(12):1605-14. 57. Sinha-Hikim I, Cornford M, Gaytan H, Lee ML, Bhasin S. Effects of testosterone supplementation on skeletal muscle fiber hypertrophy and satellite cells in community-dwelling older men. J Clin Endocrinol Metab. 2006 Aug;91(8):3024-33. |



Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun