Life Extension Magazine®

Bioidentical Hormones:
Big Pharma and the FDA have launched a disinformation campaign to frighten women away from bioidentical estrogens and pro-gesterone. In response, Life Extension® commissioned a landmark White Paper to examine every scientific study relating to estrogen and progesterone replacement therapy. The hard facts reveal the lethal side effects of FDA-approved hormone drugs. This is in stark contrast to the remarkable safety and efficacy profile of individually compounded bioidentical progesterone and estriol-based creams.
Scientifically reviewed by: Dr. Gary Gonzalez, MD, in October 2024. Written by: Life Extension Editorial Staff.
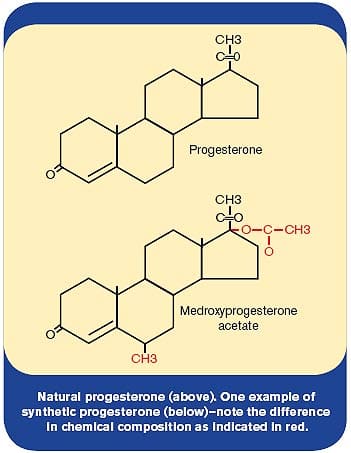
As women enter the menopausal years, they face a difficult decision. Their bodies’ production of estrogen, progesterone, and other hormones needed to maintain youthful vitality rapidly declines. While individual effects of menopause vary widely, many women suffer because their bodies no longer produce sex hormones at sufficient levels required to optimally sustain critical physiological processes. Depression, irritability, and short-term memory lapses are common menopausal complaints, along with hot flashes, night sweats, insomnia, and weight gain. Health problems encountered during menopause may adversely affect a woman for the rest of her lifetime in the absence of appropriate hormone replacement. Yet maturing women today are often told by their doctors to limit prolonged use of hormone drugs, only long enough to obtain relief from menopausal symptoms and then no more. Unfortunately, this advice fails to recognize the critical differences between hormone drugs foreign to women’s bodies and hormones identical to those naturally produced by women’s bodies. The understandable, factual concern espoused by many mainstream doctors is that FDA-approved estrogen-progestin hormone drugs have been shown to increase the risk of cancer and cardiovascular disease. The dilemma facing aging women is that their bodies may still benefit from youthful hormone levels, but many of their doctors say “no.” There is, in fact, a body of scientific evidence indicating that natural progesterone (as opposed to synthetic progestin drugs) and the natural estriol form of estrogen may help protect against the very diseases caused by unnatural estrogen-progestin drugs that are foreign to the human body. Mainstream medical practitioners (many of whom prescribed unnatural hormone drugs for decades) and the FDA (which still allows these dangerous unnatural hormones to be sold) are now at the forefront urging aging women to avoid their prolonged use. Overlooked by mainstream medicine is a plethora of research findings indicating that women may more safely benefit from individualized doses of natural estrogens and progesterone over their lifetime. Almost completely ignored are lifestyle changes (such as assuring optimal vitamin D status and cruciferous vegetable intake) that may prevent and even reverse the kind of damage to cell regulatory genes inflicted by some estrogenic compounds. In this comprehensive white paper, we present data showing how women may more safely benefit from comprehensive approaches that naturally restore youthful hormone balance, while protecting aging cells against carcinogenic and atherogenic insults. The Rise and Fall of non-bioidentical Hormone Replacement TherapyFew topics have attracted as much attention in recent years as hormone replacement therapy (HRT) among postmenopausal women. For decades, physicians were prescribing patented non-bioidentical estrogen and progestin drugs such as Premarin®, Provera®, and Prempro®—to combat the symptoms of menopause. Non-bioidentical hormones are not identical in structure or activity to the hormones naturally produced within the body.
Doctors also prescribed non-bioidentical hormones to protect postmenopausal women against osteoporosis and heart disease. The rationale behind heart disease prevention was simple: during their reproductive years, women enjoy lower rates of heart disease than men, supposedly because of the protective effect of estrogen. It seemed only logical to mainstream medicine that by replacing the effect of estrogens lost at menopause with non-bioidentical hormones, women would retain some of their protection against heart disease. Unfortunately, the logic of non-bioidentical hormone replacement therapy (HRT) turned out to be fatally flawed. In 2002, the results of the Women’s Health Initiative were released early. This landmark study followed more than 16,000 women and assessed the effects of non-bioidentical hormone replacement therapy (HRT), including estrogen-only therapy and therapy that combined non-bioidentical estrogen and progestin. The findings were shocking: the estrogen/progestin arm of the study was terminated early because the non-bioidentical hormone therapy not only failed to protect against heart disease, but was shown to increase the risk of heart attack and breast cancer.1 These alarming findings led a team of researchers to boldly state in the prestigious Journal of the American Medical Association that “…the results indicate that this regimen [non-bioidentical estrogen/progestin] should not be initiated or continued for primary prevention of coronary heart disease.”1 In 2004, the non-bioidentical estrogen-only arm of the study was terminated as well because hormone replacement therapy (HRT) with conjugated equine (horse-derived) estrogen was found to increase the risk of stroke.2 These findings had an immediate impact on the millions of women taking non-bioidentical HRT, of whom up to 50% discontinued their use of non-bioidentical HRT.3 The Bioidentical Hormone Option
Bioidentical hormones have the same exact molecular structure as the hormones produced naturally within the body. The body does not distinguish between supplemental bioidentical hormones and the hormones produced within the body.4 As a result, bio-identical hormones are properly utilized, and are then able to be naturally metabolized and excreted from the body. The use of bioidentical HRT has increased during the last several years as women have sought out a more natural approach to restoring hormonal balance. Scientific Evidence Suggests Bioidentical Progesterone Does Not Increase the Risk of Breast CancerThe well-established body of literature demonstrating the harmful effects of non-bioidentical hormones might lead some women to fear taking bio-identical hormones as well. A review of the published scientific literature indicates those fears are misunderstood and unfounded. For example, thirteen studies document that non-bioidentical progestin significantly increases estrogen-stimulated breast cell replication and growth.5-17 In stark contrast; seven studies have shown that bioidentical progesterone does not induce estrogen-stimulated breast cell proliferation.18-24 Numerous studies have demonstrated an increased risk of breast cancer with the use of non-bioidentical progestins.1, 5, 25-48 However, the use of bioidentical progesterone has not been associated with an increased risk of breast cancer. Quite the contrary, research has revealed that bioidentical progesterone decreases the risk of breast cancer. In a study published in the journal Breast Cancer Research and Treatment, 80,000 postmenopausal women using various forms of HRT were followed for more than 8 years. Women who used estrogen in combination with non-bioidentical progestins had a 69% increased risk of breast cancer, compared to women who had never used HRT. However, for women who used bioidentical progesterone in combination with estrogen, the increased risk of breast cancer was completely eliminated with a significant reduction in breast cancer risk compared with non-bioidentical progestin use.49 In another investigation, these same researchers found a 40% increased risk of breast cancer for women who used estrogen with non-bioidentical progestin. Interestingly, in women who used estrogen combined with bioidentical progesterone, there was a promising trend toward a reduced risk of breast cancer, compared to women who had never used HRT.25 In essence, bioidentical progesterone appeared to protect women against the development of breast cancer. These findings confirm work done six years earlier that found a trend toward a reduced risk of breast cancer in 1,150 women using bioidentical progesterone, compared to non-users of progesterone.50
Compelling research offers further insight into natural progesterone’s ability to defend against breast cancer. In a fascinating study, scientists administered estrogen alone, bioidentical progesterone alone, estrogen plus bioidentical progesterone, or placebo to 40 women prior to surgery to remove a breast lump. The hormones were applied topically to the breast for about 12 days before surgery. As expected, when given alone, estrogen caused a 62% increase in breast cell proliferation rates compared to placebo. Conversely, the addition of bioidentical progesterone to estrogen resulted in a significant decrease in the estrogen-induced increase in breast cell proliferation rates. Even more impressive was the finding that the group receiving bioidentical progesterone alone had a 66% lower breast cell proliferation rate compared to the placebo group.18
A growing body of literature has documented a strong connection between a woman’s progesterone levels and her subsequent risk for breast cancer. A trial reported in the International Journal of Cancer in 2004 measured blood levels of progesterone in 5,963 premenopausal women. Incredibly, the analysis of the data revealed that those women with the highest blood levels of progesterone levels who had regular menses experienced an 88% decreased risk of breast cancer.51 These findings corroborate another study in which 1,083 women treated for infertility were followed for upwards of 33 years to determine their subsequent breast cancer risk. Compared to women with normal progesterone levels, those deficient in progesterone had a 540% increased risk of premenopausal breast cancer, and were 10 times as likely to die from any cancer.52 Similarly, researchers at the University of North Carolina School of Public Health measured progesterone levels in pregnant women, who were then followed for upwards of 32 years. The researchers discovered that those women with the highest blood levels of progesterone during pregnancy had a promising trend toward a lower risk of breast cancer, compared to women with the lowest levels of progesterone during pregnancy. When the researchers analyzed the risk of breast cancer in women under age 51, those with the highest progesterone levels had a staggering 70% decreased risk compared to the group with the lowest progesterone levels.53 Findings from two other investigations revealed that survival rates for breast cancer are strongly correlated with the patient’s progesterone levels at the time of surgery.54,55 One study noted that 65% of women with a progesterone level of 4.0 ng/mL or more on the day of their surgical treatment of node-positive cancer were alive 18 years later, while only 35% of women with low progesterone levels on the day of surgery were still living after 18 years. The scientists noted that progesterone lowers the expression of vascular endothelial growth factor, which promotes the increase in new blood vessels (angiogenesis) that is essential for tumor growth. These scientists concluded: “This study has confirmed that a raised level of progesterone at the time of tumor excision is associated with an improvement in prognosis for women with operable breast cancer.”55 Estriol and the Risk of Breast CancerWhen discussing estrogen it is important to note that “estrogen” is an umbrella term for many different estrogens including estriol, estrone, and estradiol. All three of these estrogens are produced in the body and have physiological effects. In the past, estriol was believed to have little physiological significance due to its weak estrogenic activity when compared with estrone and estradiol. Nonetheless, research suggests that estriol’s weakness may confer certain beneficial effects in contrast with more potent estrogens. The benefits of estriol may, in part, be explained by its mixed pro-estrogenic and anti-estrogenic effects. Scientists investigated the mixture of stimulating and non-stimulating effects produced by estriol on estrogen receptors. When estriol is given together with estradiol, the estradiol-specific stimulation to cells is decreased.66 This little-appreciated scientific fact helps to explain how estriol can reduce pro-carcinogenic effects of more powerful estrogens like estradiol. Experimental studies suggest that estriol has a protective effect against radiation-induced cancer of the breast.67
A greater understanding of estriol’s anti-estrogenic activity becomes apparent when examining the differing effects of the three primary estrogens upon estrogen receptor binding activity. There are two distinct estrogen receptors that estrogen hormones bind on breast cells: estrogen receptor alpha and estrogen receptor beta.68-73 The binding of estrogen hormones to estrogen receptor alpha promotes breast cell proliferation, which can lead to breast cancer development. Conversely, the binding of estrogen hormones to estrogen receptor beta inhibits breast cell proliferation and prevents breast cancer development.74-79 Estrone and estradiol bind to and activate estrogen receptor alpha, thereby explaining the known breast cancer-promoting effects of these two hormones.80,81 Estriol, on the other hand, binds to and activates estrogen receptor beta.80,81 This critical fact helps to explain estriol’s anti-estrogen activity, which led a noted researcher in hormone replacement therapy to state: “This unique property of estriol, in contrast to the selective ER [estrogen receptor] alpha binding by other estrogens, imparts to estriol a potential for breast cancer prevention, while other estrogens [estrone and estradiol], would be expected to promote breast cancer… Because of its differing effects on ER alpha and ER beta, we would expect that estriol would be less likely to induce proliferative [potential cancerous growth] changes in breast tissue and to be associated with a reduced risk of breast cancer.”82 A study published in the International Journal of Cancer in 2004 reported on the use of hormone replacement therapy (HRT) and breast cancer incidence in 31,451 postmenopausal women. The analysis of the data determined that women who used estriol did not have an increased risk of breast cancer, compared to women who never used HRT.83 Additional evidence of estriol’s safety was provided by a study that compared use of HRT in 3,345 women over age 50 with breast cancer to 3,454 women without breast cancer. Those women who used non-bioidentical estrogen had a risk of breast cancer that was double that of women who never used HRT. However, women who used low-dose oral or topical estriol did not have an increased risk of breast cancer, compared to women who never used HRT.33 Intriguing research has uncovered that estriol might confer a protective effect against the development of breast cancer. This was demonstrated in an unpublished 35- to 40-year prospective study of 15,000 women who had pregnancies between 1959 and 1967. The women had samples of their blood frozen for 30 years or more. In 1997, the researchers thawed the blood and measured hormone levels to determine the relationship between estriol levels during pregnancy and subsequent incidence of breast cancer. The researchers found that breast cancer risk was reduced by 58% among women with the highest estriol levels compared to those with the lowest estriol levels.84 This study has important implications, as the findings suggest that having optimal estriol levels can play a pivotal role in the prevention of breast cancer.
| |||||||||||||||


Estriol and Uterine CancerThe increased risk of uterine cancer in users of non-bioidentical estrogen is well-established in the scientific literature.85-87 In contrast, the use of topical lower-potency estriol is not associated with an increased risk of uterine cancer.88 Other studies have demonstrated that the use of intravaginal estriol has low risk. A review of 12 studies determined that the use of intravaginal estriol did not result in endometrial proliferation (abnormal overgrowth of the cells lining the uterus with the potential to become cancerous). The authors of the study concluded that “single daily treatment with intravaginal estriol in the recommended doses in postmenopausal women is safe and without an increased risk of endometrial proliferation or hyperplasia.”89 Although several studies suggest that the oral route of administration of estriol appears relatively safe over the short term (e.g., less than five years), topical application is preferred for long-term use. For example, one study found an increased risk of endometrial atypical hyperplasia and endometrial cancer with oral use of estriol, but not with topically applied estriol over a five-year period. Compared with individuals who did not take estriol, those who took oral estriol for at least five years had a significantly greater risk of uterine cancer.88 Women using topical estriol for at least five years did not have any increased risk.88 As you will read in the “Safety” box, several studies suggest that the use of topical bioidentical progesterone cream may further reduce the risk to the endometrium.90-92 Safety ConcernsMost of the research cited in this article used oral estrogen as the route of administration. For enhanced safety, topical estriol would be a better choice. Several studies have shown that transdermal and transmucosal estrogen confers fewer health risks than oral estrogen.88,93-96 Clinical experience of many doctors over the past 20-30 years suggests that transdermal and transmucosal estrogen is also more effective for some women’s symptoms.97 One reason for this difference is the ‘first-pass effect’—meaning that orally ingested drugs are often first metabolized in the liver, before having any activity in the body. Orally ingested estrogen hormones are among these drugs that are first metabolized in the liver before exerting their effects in the body. Physicians experienced in hormone replacement often observe that women treated with oral estrogens show high levels of estrogen metabolites in 24-hour urine specimens, suggesting that most of the orally ingested hormones are metabolized and then excreted.64,98 In addition, several studies suggest that bioidentical estrogen has fewer health risks when given with low doses of bioidentical progesterone.99,100 Bioidentical Progesterone and Cardiovascular HealthThe Women’s Health Initiative, a large randomized clinical trial, demonstrated that the addition of non-bioidentical progestins to non-bioidentical estrogen therapy resulted in a substantial increase in the risk of heart attack and stroke.1,26 Numerous studies, on the other hand, document that bioidentical progesterone has beneficial effects on cardiovascular health. In one trial published in the Journal of the American College of Cardiology, researchers studied postmenopausal women with a history of heart attack or coronary artery disease. The women were given estrogen in combination with either bioidentical progesterone or non-bioidentical progestin. After 10 days of treatment the women underwent exercise treadmill tests. Compared to the non-bioidentical progestin group, the amount of time it took to produce myocardial ischemia (reduced blood flow to the heart) on the exercise treadmill was substantially improved in the bioidentical progesterone group.131
The risk of a blood clot is a serious concern with the use of unnatural estrogen replacement therapy, especially by the oral route. This risk doesn’t occur when bioidentical progesterone is added to the mix. One investigation compared the risk of blood clots in postmenopausal women taking bioidentical progesterone to the risk in women taking non-bioidentical progestin. The group of women who used non-bioidentical progestin in combination with estrogen had a startling 290% greater risk of blood clots, compared to the group who never used HRT. In a reversal of fortunes, the group receiving bioidentical progesterone in combination with estrogen had a 30% decreased risk of blood clots, compared to women who never used HRT.132 Atherosclerosis (hardening of the arteries) is the leading cause of heart disease. Several studies have determined that non-bioidentical progestin promotes the formation of atherosclerosis.133-135 The story is quite different for bioidentical progesterone, where multiple animal studies have shown that bioidentical progesterone inhibits the process of atherosclerosis.135-137 To illustrate, scientists fed postmenopausal monkeys a diet which is known to cause atherosclerosis for 30 months. The scientists then divided the monkeys into groups that received estrogen alone, estrogen plus non-bioidentical progestin, or a control group that did not receive hormones. The control group developed substantial atherosclerotic plaque. The administration of estrogen resulted in a 72% decrease in atherosclerotic plaque, compared to the control group. Treatment with non-bioidentical progestin yielded disturbing results. The group that received estrogen combined with non-bioidentical progestin had a similar amount of atherosclerotic plaque as the control group, meaning that non-bioidentical progestin completely reversed estrogen’s inhibitory effects on the formation of atherosclerosis.135 In contrast, when the same investigators administered bioidentical progesterone along with estrogen, no such inhibition of estrogen’s cardiovascular benefit was seen.138
Bioidentical Progesterone and HDLHigh-density lipoprotein (HDL) functions to remove cholesterol from the arterial wall and thus helps protect against the development of atherosclerosis.139 Low HDL is a proven risk factor that contributes to heart disease. Non-bioidentical progestin is known to cause reductions in HDL levels.140-145 One mechanism by which bioidentical progesterone enhances cardiovascular health is its ability to maintain or even increase HDL levels in women receiving estrogen replacement therapy.141,142,146-148 In one study published in the Journal of the American Medical Association, 875 postmenopausal women were randomized to receive estrogen alone, estrogen combined with non-bioidentical progestin, estrogen combined with bioidentical progesterone, or placebo. The results demonstrated that the group receiving bioidentical progesterone experienced significantly higher HDL levels than the group receiving non-bioidentical progestin.141 These results confirm earlier preliminary data provided by researchers who administered estrogen combined with either non-bioidentical progestin or bioidentical progesterone to postmenopausal women. The use of non-bioidentical progestin resulted in an undesirable 15% decrease in HDL levels, whereas there was no decrease in HDL levels in those patients prescribed bioidentical progesterone.142 Estriol and Cardiovascular HealthGrowing evidence suggests that estriol may offer benefits to the cardiovascular system. For instance, Japanese scientists found that a group of menopausal women given 2 mg/day oral estriol for 12 months had a significant decrease in both systolic and diastolic blood pressure.149 Another study compared the use of oral estriol at a dose of 2 mg/day for 10 months in 20 postmenopausal and 29 elderly women. Some of the elderly women had decreases in total cholesterol and triglycerides and an increase in beneficial HDL.150 To examine the effects of estriol on atherosclerosis, researchers conducted an experiment in which female rabbits were fed a high cholesterol diet with or without supplemental estriol. The rabbits had their ovaries removed surgically to mimic menopause. Remarkably, the group receiving estriol had 75% less atherosclerosis than the group fed the high cholesterol diet alone (without estriol).151 | |||||||||||||||||||||||||||||||



Bioidentical Progesterone vs. non-bioidentical Progestin for the Treatment of Menopausal SymptomsFour head-to-head studies comparing bioidentical progesterone to non-bioidentical progestin reported that women experienced greater satisfaction, improved quality of life, and fewer side effects when they were switched from non-bioidentical progestin to bioidentical progesterone. In a landmark study, researchers at the Mayo Clinic studied 176 menopausal women receiving hormone replacement therapy. All of these women had previously taken hormone replacement therapy with non-bioidentical progestin, but were switched at a later date to bioidentical progesterone. The findings across the board showed that women had substantially greater improvement in their symptoms when using bioidentical progesterone, compared to non-bioidentical progestin. Sixty-five percent of the women believed that HRT combined with bioidentical progesterone was better than HRT combined with non-bioidentical progestin. The beneficial effects of bioidentical progesterone compared to non-bioidentical progestin included a 30% reduction in sleep problems, a 50% reduction in anxiety, a 60% reduction in depression, a 25% reduction in menstrual bleeding, a 40% reduction in cognitive difficulties, and a 30% improvement in sexual function. Eighty percent of women in the study reported overall satisfaction with the bioidentical progesterone formulation.152 The results of this study provide evidence of the superiority of bioidentical progesterone over non-bioidentical progestin in the treatment of menopausal symptoms. Further research supports the use of bioidentical progesterone in preference to non-bioidentical progestin. One study of menopausal women receiving HRT found that those receiving non-bioidentical progestin experienced greater vaginal bleeding and breast tenderness than those receiving bioidentical progesterone.153 Two other studies with menopausal women also determined that HRT with non-bioidentical progestin was associated with greater vaginal bleeding compared to those receiving bioidentical progesterone.154,155 Bioidentical progesterone also offers improvements in quality of sleep and cognitive function compared with non-bioidentical forms of the hormone.156,157 Estriol and Menopausal SymptomsStudies have shown estriol to be effective in the treatment of menopausal symptoms. In one investigation, 52 postmenopausal women were given 2 mg, 4 mg, 6 mg, or 8 mg/day of oral estriol for six months. In all patients, vasomotor symptoms of menopause (such as hot flashes) were decreased. The most improvement was experienced by women taking the highest dose of 8 mg. There were no signs of endometrial hyperplasia confirmed by endometrial biopsy over the six-month treatment period. Mammograms were obtained on six of the patients who had breast hyperplasia at the study’s outset, and no further changes were seen.158
In another trial, researchers studied the safety of estriol in the treatment of menopausal symptoms. Fifty-three women with either surgically induced or natural menopause were given 2 mg of oral estriol/day for 12 months. Endometrial biopsy and breast ultrasound found normal results in all women. The authors concluded that over a 12-month period, “estriol appeared to be safe and effective in relieving symptoms of menopausal women.”149 A 5-year study demonstrated the successful use of estriol in the treatment of menopausal symptoms. In 71% of the participants, hot flashes and sweating were eliminated completely, while in 21% they were weaker and occurred less frequently. Depressive moods were abolished in 24% of the women and were reduced in severity in another 33%. Reductions in forgetfulness, loss of concentration, irritability, and heart palpitations were also recorded, while the number of women who experienced migraine headaches dropped by two-thirds. Thrombophlebitis occurred in two patients and there were two cases of mammary cancers, which the investigators did not believe were related to the estriol treatment.159 Given the wealth of data demonstrating the superiority of bioidentical HRT over non-bioidentical HRT, a noted researcher in hormone replacement therapy proclaimed that “Physiological data and clinical outcomes demonstrate that bioidentical hormones are associated with lower risks, including the risk of breast cancer and cardiovascular disease, and are more efficacious than their… animal-derived [non-bioidentical] counterparts. Until evidence is found to the contrary, bioidentical hormones remain the preferred method of HRT.”82 Beyond Menopause: Enhancing Health with Bioidentical HormonesThe benefits of bioidentical hormones are by no means limited to the relief of menopausal symptoms. Maturing women can reap long-term health benefits by restoring youthful hormonal balance with the use of bioidentical hormones. The Life Extension® has written extensively regarding the importance of maintaining optimal hormone balance as we age in order to ensure optimal health. Estriol Increases Bone Mineral DensityOne of the unfortunate consequences of decreased estrogen production in maturing women is the loss of bone density, with the potential to develop osteoporosis. A Japanese study involving 75 postmenopausal women found that after 50 weeks of treatment with 2 mg/day of oral estriol cyclically and 800 mg/day of calcium lactate, women had an increase in bone mineral density with no increased risk of endometrial hyperplasia (uterine tissue overgrowth that may precede cancer).160 In a second study emanating from Japan, researchers treated postmenopausal and elderly women with 2 mg/day of oral estriol and 1,000 mg/day of calcium lactate versus 1,000 mg/day calcium lactate alone. Bone mineral density significantly increased in women who received estriol, while the women who did not take estriol experienced a decrease in bone mineral density.150
Similar research has confirmed these findings. In this investigation, 25 postmenopausal women were given either 2 mg/day of estriol plus 2 gram/day of calcium lactate, or 2 grams/day of calcium lactate alone for one year. Bone mineral density was significantly reduced in the group that received calcium alone (without estriol). In contrast, the group that received estriol plus calcium experienced a 1.66% increase in bone mineral density after one year. Furthermore, biochemical markers of bone resorption were significantly decreased in the estriol group. “These data indicate that the acceleration of bone turnover usually observed after menopause was prevented by treatment with E3 [estriol],” the authors of this study noted.161 The most dramatic improvements in bone density were reported by scientists in the Journal of Bone and Mineral Metabolism. In this study, 41 women over age 49 with decreased bone density received either 2 mg/day estriol orally with calcium, or calcium alone for 10 months. The group receiving estriol experienced a striking 5% increase in bone density, while the group that did not receive estriol experienced a 3% decrease in bone density.162 Estriol Enhances Sexual and Urinary HealthPostmenopausal women often suffer from urinary incontinence or recurrent urinary tract infections caused in part by hormone deficiencies. In a prospective, randomized, placebo-controlled study, 88 women were given 2 mg intravaginal estriol suppositories (once daily for two weeks, then twice weekly for six months) or placebo. Of the women in the estriol group, 68% reported improvement in symptoms of incontinence, while only 16% improved in the placebo group.163 In another randomized, double-blind, placebo-controlled trial, women with recurrent urinary tract infections were given either intravaginal estriol cream (containing 0.5 mg estriol, once daily for two weeks, then twice weekly for eight months) or placebo. Incredibly, the incidence of urinary tract infection was reduced by 91% in the estriol group compared with placebo.164 The substantial decrease in estrogen that occurs after menopause can lead to a condition called atrophic vaginitis. The symptoms, which include vaginal dryness, vaginal burning, and painful sex can be quite bothersome for aging women. Fortunately, the use of estriol can offer relief for women suffering from these symptoms. One group of researchers, who prescribed oral estriol to 62 postmenopausal women with vaginal symptoms in a double-blind and placebo-controlled fashion, concluded that “estriol has a remarkably beneficial effect on the vaginal epithelium.”165 Another group of researchers prescribed an estriol cream for women with atrophic vaginitis. After 4 weeks of treatment, the researchers noted that “atrophy of vaginal epithelium and chronic vaginitis stopped or significantly decreased… The subjective complaints relating to the estrogen deficiency (vaginal burning and dryness, itching, dyspareunia [painful sex] and urinary dysfunctions) ceased. Side-effects and complications during the treatment were not found.”166 In a study conducted in Japan, oral estriol (2 mg/day) was administered to 59 postmenopausal women complaining of vaginal itching or discharge. After 14 days of treatment, substantial improvements were noted in the women’s vaginal flora. The authors of the study concluded: “Estriol… has the potential to be highly useful for the treatment of atrophic vaginitis.”167 Estriol Promotes Youthful SkinOne reason that facial skin “shrivels” as we age is that our natural hormone production markedly declines. To make matters worse, blood microcirculation to our skin is reduced as we grow older, thereby depriving our skin of the small amount of natural hormones our body still makes.168 A large number of published scientific studies reveal that estrogen exerts potent anti-aging effects on the skin.169-178 The topical application of natural estrogen can produce dramatic improvements to the skin without systemic absorption concerns. The deficiency of estrogen that characterizes menopause exacerbates the effects of both normal and environmentally-induced skin aging. According to the findings of a scientific study published in 2007, “Estrogens prevent skin aging. They increase skin thickness and improve skin moisture.”178 Another recent study came to the same conclusion, i.e. “skin aging can be significantly delayed by the administration of estrogen.”170 A critical mechanism by which estrogen maintains a youthful plump appearance is by increasing the synthesis of collagen, which is the skin’s underlying support structure. Collagen atrophy is a major factor in skin aging. There is a strong correlation between skin collagen loss and estrogen deficiency at menopause.169 Skin aging, especially in the face, is associated with a progressive increase in sagging tissues and a reduction in elasticity. In menopausal and postmenopausal women, estrogen administration increases collagen content, dermal thickness and elasticity, while decreasing aging dry skin.169,172
Estrogens exert significant effects on skin physiology by modulating the effects of key epidermal and dermal cells.170 In fact, the skin is an important estrogen-responsive tissue, and without the growth promoting effects of estrogen, it literally withers away.171 The very thin skin observed in the elderly can be directly correlated to a lack of estrogens needed to generate collagen and maintain skin thickness.171 Topical estrogen application has been shown to be safe and effective in preventing skin aging. In a study published in February 2007, a group of women who were already taking oral estrogen drugs were given a topical 0.01% estrogen cream. After only four months, both dermal and epidermal thickness was enhanced, as were dermal collagen levels. This study showed that topical estrogen application provided rapid and definitive anti-aging effects even in women who had high systemic estrogen blood levels.172 The significance of this study is that it shows how quickly a small amount of estrogen delivered directly into the skin induces profound anti-aging effects. A six-month study of perimenopausal women was conducted at the University of Vienna in Austria comparing the topical application of estriol and estradiol creams. The doctors found that skin symptoms of aging improved, and that those treated with estriol obtained superior results in decreased wrinkle depth, with no systemic hormonal side effects noted.173 In another study, twenty women with mild crow’s feet, rough-textured skin, and moderate skin tone with some blotching and imperfections applied a topical solution containing estriol with 15 other ingredients on only one side of their faces over a six-week period. All of the subjects reported that their skin texture on the treated side was smoother and that the quality of their skin had improved, while 90% and 80% said that the moisture content and elasticity of their skin had increased, respectively, giving them a healthier and younger-looking appearance. Clinical assessments showed a baseline improvement of 19% increase in elasticity and 9% increase in moisture in the skin after just one week.179 | ||||



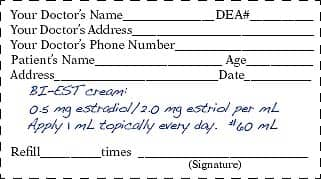
How Bioidentical Estrogen-Progesterone Is PrescribedCurrently, widespread commercial availability of individually tailored bioidentical hormone prescriptions is lacking. As a result, many physicians utilize compounding pharmacies to dispense bioidentical hormone prescriptions for their patients. To obtain the phone number of a compounding pharmacist, call 1-866-864-3027. Most practitioners use the level of estradiol in women’s blood, along with an assessment of the patient’s clinical symptoms to prescribe the initial dose of bioidentical estrogen. The estradiol blood level must be considered in context to the other hormones such as progesterone. A health care practitioner may also measure levels of estrone and estriol to obtain a more comprehensive assessment of a woman’s estrogen status. In menopause, a woman typically has an estradiol blood level of 0-19 pg/mL. With the use of bioidentical estrogen topical cream (e.g., compounded estriol and estradiol), the blood estradiol level may go to 100 pg/mL or higher, which indicates to the prescribing doctor that the compounded estrogen formula is being absorbed and has increased the patient’s estradiol level to a more youthful range. If the patient reports that her menopausal symptoms have resolved, most practitioners would continue the patient on the current program and conduct periodic follow-up. If, however, the patient is still having symptoms, the bioidentical estrogen topical cream dose can be increased or additional tests ordered such as the total estrogen blood test or a urinary estrogen test to assess other estrogens and their associated metabolites. Based on findings from these tests, a more precise dose of estriol, estradiol, progesterone, and sometimes testosterone can be prescribed. A typical starting dose for bioidentical estrogen topical cream might read as:
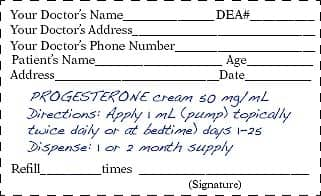
Please note that this is a general suggestion for an initial prescription. A physician experienced in bioidentical hormone replacement will tailor the prescription to the person’s individual needs. The bioidentical estrogen topical cream dose can be increased when severe symptoms of estrogen deficiency are present. Women given estrogen replacement should also be prescribed natural progesterone (in contrast to synthetic progestin drugs like Provera®) in a dose that achieves a youthful balance. Natural progesterone produces many benefits when properly balanced with estrogen. The typical dose for topical progesterone cream may vary between 50-200 mg, depending upon a woman’s unique, individual biochemical needs. A typical starting dose for over-the-counter (OTC) progesterone cream is one-quarter teaspoon of a 2.5% strength progesterone cream applied to a different part of the body twice each day:
The dose can be adjusted up or down depending on a woman’s symptoms and her response to treatment. If using natural progesterone cream from a pharmacy, a prescription could be written as follows for a postmenopausal woman:
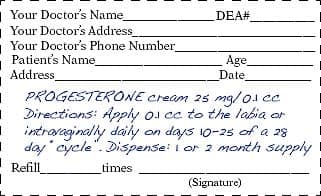
A prescription for a premenopausal woman could also read:
Some physicians will prescribe topical progesterone in a similar way to estrogens, in milligrams per fraction of a cubic centimeter (cc).These dosages are “pressed out” of a syringe onto the skin, and have the dual advantages of more precise dosage adjustment and smaller volume of “crème,” which is less likely to make a mess on clothing. A blood level target to strive for in aging women might be:
Before a prescription for bioidentical hormones can be written, it is important to have a baseline blood test so the doctor knows what dose of bioidentical estrogens, progesterone, and possibly testosterone may be needed. To order a comprehensive Female Blood Test Panel that includes estradiol, progesterone, and free testosterone, call 1-866-864-3027. Although this paper focuses on bioidentical estrogen and progesterone, it is important to also address testosterone levels in order to achieve optimal hormonal balance. Although testosterone is thought of as a male hormone, it plays an important role in women’s health as well. Testosterone levels decrease in women as they age. Low testosterone in women can have a negative impact upon sex drive, mood and well-being, bone and muscle mass, and cardiovascular health.180-183 A physician experienced in bioidentical hormone therapy will measure testosterone levels in women, and prescribe bioidentical testosterone if levels are low. Correcting low testosterone in women usually requires a 150 to 300 mcg patch or an individually prescribed testosterone cream.184 Since DHEA (dehydroepiandrosterone) can convert to testosterone in a woman’s body, a woman with low testosterone might be able to increase her testosterone level by taking 15 mg to 25 mg a day of DHEA, which is available as a low cost dietary supplement.185 Too much free testosterone in an aging woman induces abdominal weight gain,186,187 as does a deficiency of estradiol.188-191 Progesterone may be weight-neutral,192 though some complementary practitioners claim it helps facilitate weight loss. Some doctors seek to increase progesterone levels up to 15 ng/mL. The overall objective is to achieve a more youthful hormone balance to improve the patient’s appearance, state of health, and well-being. The use of estrogen drugs is contraindicated in women with existing estrogen receptor-positive cancer.
Why Skeptics Are Still Concerned About EstriolBased on what you have read so far, topical estriol appears to be a safe and optimal antidote to correct estrogen deficits. Not everyone agrees, however. Some doctors are concerned that the long-term use of estriol might increase cancer risk. These doctors seem unaware of the evidence indicating that estriol may reduce breast cancer incidence, or of documented methods to protect against estrogen-induced side effects.
Unlike cynics who view any form of estrogen as a carcinogen, the Life Extension Foundation® has examined the published studies to ascertain what real risks may exist when supplementing with estriol (and other estrogens). One concern about all estrogens is that they undergo alterations in the body that can result in these estrogens cascading into either pro-carcinogenic or anti-carcinogenic compounds. The good news is that one can affect whether estrogens increase or decrease cancer risk via their diet and/or supplement intake. Skeptics view estriol supplementation in a vacuum, as if women will take estriol and do nothing else. You have already read extensive documentation about how natural progesterone significantly protects against estrogen-induced cancers. What you will read next is what all women should do to reduce breast and other cancer risk (whether or not they take supplemental estrogen). These recommendations are based on large human population studies showing huge reductions in cancer risk and specific protective mechanisms against estrogen’s negative pathways when vitamin D, cruciferous vegetables, soy, D-glucarate, and/or plant lignans are consumed. These cancer rate reductions also occur when red meat, high-fat dairy, and other deleterious foods are reduced or eliminated from the diet. Anticancer Nutrients That Complement Bioidentical HRTCritical Importance of Vitamin DYoung women (under age 30) almost never develop breast cancer. As women age, their cell growth-regulatory genes accumulate mutations. As our bodies age, we become less proficient at rapidly repairing (or removing) damage to the cells and tissues of our bodies. When genes that regulate cell division undergo mutation, the result can be uncontrolled cell propagation that results in tumor formation. Aging women experience a dramatic rise in cancer incidence, even as their estrogen levels plummet. In the presence of changes to genes involved in the growth and proliferation of breast tissue cells, estrogen can promote cancer cell propagation. The good news is that the ingestion of vitamin D, cruciferous vegetables, and other compounds can prevent and help repair gene mutations and thus reduce cancer risk. All women (including those who maintain youthful estrogen levels) should make sure they are ingesting optimal amounts of vitamin D and other compounds that favorably alter gene expression.
Vitamin D confers significant protective effects against breast cancer. Laboratory studies have shown that vitamin D suppresses growth of breast cancer by 1) blocking signals that stimulate cancer cell growth, 2) by enhancing signals that inhibit cancer cell growth, and 3) by favorably altering gene regulators of the cell cycle.195-198 This three-pronged effect of vitamin D can prevent mutated cells from becoming malignant and even induce cancer cell death (apoptosis). Studies have found a strong correlation between blood levels of vitamin D and the risk of breast cancer. A case-control study comparing 1,394 postmenopausal breast cancer patients with 1,365 controls showed that low blood levels of vitamin D were significantly related to breast cancer risk. In fact, women with the highest levels of vitamin D had a nearly 70% reduction in their risk of breast cancer, compared to women with the lowest vitamin D levels.199 Similar research examining the relationship between blood levels of vitamin D and breast cancer risk revealed that women with blood vitamin D levels of approximately 52 ng/mL had a 50% lower risk of breast cancer compared with women who had vitamin D levels below 13 ng/mL.101 In a one report, the effects of administering 1,100 IU a day of vitamin D (with calcium) was evaluated in 1,180 postmenopausal women.127 After only four years, the risk of developing any cancer was 60% lower in the vitamin D (and calcium) group, compared with those who received calcium only. The scientists then performed a more detailed analysis of the data. When excluding cancers diagnosed in the first year of the study, which would have included pre-existing cancers present at the time participants began taking vitamin D, they found an astounding 77% reduction in cancer incidence in the group receiving vitamin D, compared with placebo. Ensuring vitamin D blood levels over 50 ng/mL is a critical step in reducing cancer risk. Life Extension® is finding that many people require 5,000 IU a day of supplemental vitamin D3 and higher to achieve these optimal blood levels. These doses have been shown to be both effective and safe in human trials.200,201 The heavier one is, the more supplemental vitamin D they often require. (Note that vitamin D status in the body is measured as serum 25-hydroxyvitamin D.) Cruciferous Vegetables Protect Against Tumor-Proliferating Estrogen MetabolitesScientists have identified compounds in cruciferous vegetables (broccoli, cauliflower, Brussels sprouts, cabbage, kale) that specifically neutralize dangerous breakdown products of estrogen that promote cancer growth.104,202 Cruciferous vegetable compounds also help neutralize the many carcinogens we are inevitably exposed to each day.106-109,203 One of the best-studied cruciferous vegetable compounds is called indole-3-carbinol (I3C). Women seeking to restore youthful hormone balance should make sure to obtain enough I3C from their diet or by taking standardized supplements. The reason for this is that I3C increases levels of a cancer-protective estrogen metabolite (2-hydroxyestrone), while suppressing a dangerous estrogen metabolite (16-alpha-hydroxyestrone) that promotes breast and other cancers.193,194 To emphasize the critical importance of indole-3-carbinol (I3C), please understand that aging women still produce estrogen. All the estrogen in women’s bodies (both endogenously produced and supplemental) can follow two primary metabolic pathways in the body. If estrogen is converted to 16-alpha-hydroxyestrone, then the risk of breast and other cancers is increased. If on the other hand, the estrogen is converted to 2-hydroxyestrone, then the risk for breast and other cancers is decreased.204,205 I3C can readily be obtained by eating lots of cruciferous vegetables and/or taking I3C in dietary supplement form. To confirm the theory that certain estrogen metabolites can contribute to cancer, researchers analyzed data gathered from over 10,000 Italian women over more than five years. The objective was to determine how dietary and hormonal factors influence breast cancer risk. They found that among premenopausal women, higher levels of 2-hydroxyestrone were associated with protection against breast cancer.204 This same finding has been shown in additional studies of different populations.206,207 The toxic estrogen metabolite 16-alpha-hydroxyestrone acts as a breast tumor promoter.110 By contrast, estrogen metabolized via the 2-hydroxyestrone pathway does not exhibit adverse estrogenic activity in breast tissue.110 Additionally, a form of this less active estrogen metabolite is believed to prevent the formation of blood vessels necessary to feed growing cancers, thus helping to arrest tumor growth.208 Cruciferous vegetable compounds (such as I3C) are effective in shifting estrogen metabolism to the more beneficial pathway, thus reducing levels of toxic 16-alpha-hydroxyestrone and increasing levels of protective 2-hydroxyestrone.110-112,205 This beneficial modulation of estrogen is associated with reduced risk of breast and other cancers, including cervical and head and neck cancers.106,204,205 Cruciferous vegetable compounds thus play an important role in fighting cancer. To illustrate, research conducted at the University of California at Berkeley documented that I3C in combination with the anti-estrogenic chemotherapeutic agent tamoxifen inhibited the growth of human breast cancer cells by an astounding 90%.209 Interestingly, an assay study performed at the National Cancer Institute determined that I3C was superior to 80 other natural substances with regard to anti-cancer potential.210 | ||||||||||

Soy Slashes Breast Cancer RiskFor the past decade, a controversy has raged over whether people can reduce their risk of cancer by increasing their consumption of soy foods or soy supplements. In response to the debate, a number of studies were initiated in the 1990s to ascertain soy’s effects on human health. Over the past few years, the results of these studies began to be released. While ignored by the mainstream media, the startling findings indicate that breast (and prostate) cancer risk can be cut in half if people consume more soy.125,211,212 One recent study showed that women who ate a Western-style diet, high in meats and sweets, had nearly twice the risk of developing estrogen receptor-positive breast cancer, compared with women who ate a traditional Asian diet high in soy and vegetables.125 This and other studies provide evidence that compounds found in soy have a breast cancer-preventive effect. Isoflavones derived from soy have shown great promise in providing natural protection against multiple types of cancer.114-116 Two of the best known soy isoflavones are genistein and daidzein. Isoflavones exert a number of positive biological effects on the human body, and many practitioners of integrative medicine (and even a small but growing number in mainstream medicine) now believe that consumption of soy and isoflavones can reduce the risk of many chronic diseases, including cancer, heart disease, and osteoporosis.113-116,211-217 Studies conducted in Asia found that breast cancer risk was significantly lower among Asian women who consumed large quantities of isoflavones and other soy products, compared with those who consumed less of these healthful nutrients.115 Because animal studies have shown that a diet high in soy and genistein can protect against breast, colon, and skin tumors, it seemed reasonable to think that soy could also help prevent human cancers and, in particular, breast cancer.218Yet many mainstream medical practitioners remain skeptical that something as simple as soy could have such a profound effect on human health. Soy isoflavones are correctly classified as selective estrogen receptor modulators.219 Due to their unique molecular structure, soy isoflavones can act as both estrogen receptor agonists and receptor blockers. In fact, elegant biochemical studies have shown that some isoflavones bind to the cancer-protective estrogen beta receptor six to eight-fold more readily than native estrogen.219 With this ability, soy isoflavones are thought by many to confer the beneficial effects of estrogen without its potentially dangerous side effects, especially in hormonally sensitive tissues found in both the breast and endometrium.219 Numerous studies show the potential benefits to women of incorporating soy in their diets to help prevent breast cancer. A landmark case control study of women in Singapore, involving 200 case subjects and 420 control subjects, found that women with the highest consumption of soy-based products had a markedly decreased risk of developing breast cancer.117 Finally, a very large population-based, prospective study of 21,852 Japanese women aged 40-59 found that women with the highest intake of soy isoflavones reduced their risk of breast cancer by up to 54%, compared with women with the lowest intake of soy isoflavones.115 In addition to being a chemopreventive supplement for breast cancer, soy isoflavones are also thought to be effective in warding off other types of cancer that afflict women, including endometrial cancer. A recent case control study reported the effects of soy isoflavones and other phytoestrogens on the risk of developing endometrial cancer.220 The study compared 500 women aged 35-79 who developed endometrial cancer between 1996 and 1999 with 470 age- and ethnicity-matched controls. As in studies examining the effects of isoflavones on breast cancer, this study showed that women with a higher intake of soy isoflavones had a significantly lower risk of developing endometrial cancer. Even more interesting was that the levels of isoflavones needed to provide protection against endometrial cancer were found to be much lower than the amount believed necessary to protect against breast cancer (in fact, they were the amounts that could be obtained from a healthy American-style diet). Meat Increases Breast Cancer Risk
Studies that look at human populations (epidemiological studies) have consistently shown that what we eat affects our cancer risk. Women who eat more red meat suffer higher breast cancer rates. In one of the better documented studies, postmenopausal women in China who ate a Western-style diet (which included beef, pork, and desserts) were 30% more likely to develop breast cancer than those eating a diet based on vegetables and soy. Even more startling was the finding that in women who developed estrogen receptor-positive breast tumors, those who ate the Western-style diet experienced a 90% increased risk!125 This is in stark contrast to a study that demonstrated a 52% decreased risk of breast cancer in women with the highest intake of vegetables and fruits, compared to the lowest intake.221 However, it’s not known whether meat from “free range” animals (beef, buffalo, wild game, chicken, pigs) also increases breast cancer risk. While even organically raised, grain-fed animals (like commercially raised grain-fed animals) have much more omega-6 (pro-inflammatory) fatty acids than omega-3 (anti-inflammatory) fatty acids, this ratio is reversed in meat from free-range animals, with significantly more omega-3 than omega-6 fatty acids.222 Theoretically, this much more natural ratio should be associated with lower breast (and other) cancer risk, but research still needs to be done on this point. Fish Oil and Breast Cancer RiskIn addition to fish oil’s well-known cardiovascular benefits, research has revealed that omega-3 rich fish oil might offer protection against breast cancer as well. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are the two most important components of fish oil. One investigation documented a 49% decreased risk of breast cancer in women with the highest dietary intake of omega-3 fatty acids, compared to those with the lowest intake. Furthermore, women with the highest red blood cell levels of EPA had a remarkable 73% decreased risk of breast cancer, compared to those with the lowest levels.223 A group of researchers in France compared levels of DHA in breast tissue in 241 patients with breast cancer and 88 patients with non-cancerous benign breast disease. They reported that women with the highest levels of DHA in their breast tissue had a 69% decreased risk of breast cancer, compared to women with the lowest levels of DHA in their breast tissue.224 Why Plant Foods Are So ImportantThe body is bombarded with carcinogens on a daily basis. These cancer-causing agents include pesticides, overcooked food, alcohol, food additives, tobacco, fungal mutagens, and industrial pollutants. While avoiding carcinogens is difficult, it may be possible to mitigate their lethal effects by providing the body with a specific plant extract that facilitates the detoxification and removal of these dangerous substances from the body. A compound called D-glucarate is found in grapefruit, apples, oranges, broccoli, and Brussels sprouts.225,226 D-Glucarate has been shown to protect against cancer-causing agents by supporting detoxification and removal of dangerous chemicals, and also by protecting against the mutating effects that these carcinogens induce on cellular DNA.227 There are several mechanisms by which the body detoxifies itself. One way of guarding against toxic overload involves a pathway of detoxification in the body whereby carcinogens are combined with water-soluble substances, thus making them more easily removed from the body. This process is called glucuronidation, and D-glucarate has been shown to support this important detoxification mechanism.227 D-Glucarate functions by inhibiting the beta-glucuronidase enzyme, thus protecting the critical “glucuronidation” detoxification mechanism. One example of the importance of glucuronidation can be seen in the risk factors for breast cancer. Excess levels of 16-alpha-hydroxyestrone and beta-glucuronidase enzyme activity are associated with an increased incidence of breast cancer.228 D-Glucarate is thought to decrease estrogen’s effects by favorably affecting estrogen’s metabolism and elimination. Research studies have shown that D-glucarate inhibits breast tumor incidence.118,119 One study in rats that already had breast cancer showed that oral D-glucarate administration resulted in a 50% inhibition of beta-glucuronidase, which led to a 30% reduction in mammary tumor growth during the promotion stage and a four-fold reduction in the absolute number of tumors.229 Another report showed a more than 70% decrease in mammary tumor development in rats exposed to carcinogens that were also administered D-glucarate.120 Still another study looked at the effects of D-glucarate on the initiation and promotional stages of mammary cancer. The results showed a reduction of 28% during the initiation stage, while cell replication was reduced by 42% during the promotion stage.121 Inhibition at the initiation stage is a very important part of D-glucarate’s actions, as it reduces the risk that cancer will even start. Eating lots of the right fruits (grapefruit, apples, cherries) and vegetables (broccoli, Brussels sprouts) supplies the body with D-glucarate, though it is also available in dietary supplements designed to support breast health. How Lignans Protect the BreastA number of published studies indicate that dietary lignans may protect against cancer by favorably altering estrogen metabolism, inhibiting angiogenesis, and inducing cancer cells to self destruct.122,123 The greatest support for a role of lignans in cancer prevention has been shown for premenopausal breast cancer. Researchers in New York assessed breast cancer risk and dietary lignan intake in more than 3,000 women, including about 1,100 patients with confirmed breast cancer and approximately 2,000 cancer-free women who served as controls. The scientists determined that premenopausal women with the highest lignan intake had a 44% reduced risk of developing breast cancer.122 Scientists in Italy suggest a mechanism for the protective effect. Their research indicates that higher blood levels of a phytoestrogen called enterolactone—the primary lignan derived by the body from flaxseed—are associated with a lower risk of breast cancer. Conversely, the researchers noted, “values of serum enterolactone were significantly lower in women who subsequently developed breast cancer,” leading them to conclude that the enterolactone “had a strong protective effect on breast cancer risk.”123
Scientists at the University of Toronto reported that flax lignans can slow down the growth of breast cancer in women. Thirty-two women awaiting surgery for breast cancer were randomized to receive a muffin containing 25 grams of flaxseeds or a muffin that did not contain flaxseed (control group). Analysis of the cancerous tissue after surgery revealed that markers of tumor growth were reduced by 30%-71% in the flaxseed group, while the control group did not experience any reduction in markers of tumor growth. The scientists concluded that “dietary flaxseed has the potential to reduce tumor growth in patients with breast cancer.”230 Lignans may also protect against endometrial cancer, a condition associated with prolonged exposure to unopposed estrogens (this means estrogen administered without progesterone). Researchers in California assessed lignan intake and cancer status among nearly 1,000 women in the San Francisco area and determined that women with the highest dietary lignan intake experienced a promising trend toward a lower risk of developing this carcinoma of the uterine lining.220 The relationship between lignans and endometrial cancer risk reduction was slightly stronger among postmenopausal women. Based on a lot of favorable publicity, health-conscious people are increasingly adding flaxseed to their diet for the purpose of obtaining the beneficial lignans. Highly concentrated lignan extracts are also available in dietary supplements. Green Tea’s Anti-Cancer EffectsGreen tea is rich in plant compounds known as polyphenols. The most active group of green tea polyphenols is the catechins, particularly epigallocatechin gallate (EGCG). Copious evidence supports a role for these compounds in preventing breast cancer. In laboratory studies, green tea polyphenols and EGCG have been shown to suppress the growth and reproduction of human breast cancer cells.231,232 Of even greater interest, these beneficial compounds in green tea delay the appearance of tumors in mouse models of breast cancer and cut down on the total tumor burden (amount of cancer in the body) when human breast cancer cells are injected into laboratory mice.232,233
Other exciting benefits of green tea include inhibition of vascular endothelial growth factor (VEGF) production,233,234 which cuts off the blood supply needed for tumor growth; down-regulation of estrogen receptor-alpha function in breast cancer cells;235 reduction of tumor invasiveness;233 and increased apoptosis, or programmed cell death, in cancer cells.236 One experiment showed that EGCG, 50-100 mg/kg/day, added to the drinking water of female mice, inhibited growth of breast cancer. After five weeks of EGCG treatment, the weight of breast tumors was reduced by 68% in mice consuming EGCG daily.237 But green tea’s benefits aren’t restricted to animal or laboratory models. An investigation found a 47% decreased risk of breast cancer in women who drank at least 3 cups per day of green tea, compared to those who did not consume any green tea.238 The medical establishment questions the use of bioidentical hormones out of concern about cancer risks. Earlier in this article, we outlined persuasive data showing the anti-cancer properties of estriol and natural progesterone. When factoring in the potent anti-cancer effects that occur in response to consuming healthy foods (such as broccoli and soy) and supplements (such as vitamin D and fish oil), while avoiding carcinogenic foods (such as sugar and well-done meat), the argument that maturing women should forever be denied their full complement of natural sex hormones does not stand up to scientific scrutiny. | ||||||



ConclusionDr. Kent Holtorf, MD, a specialist in bioidentical hormone therapy and anti-aging medicine stated: “A thorough review of the medical literature clearly supports the claim that bioidentical hormones have some distinctly different, often opposite, physiological effects to those of their synthetic [non-bioidentical counterpart] hormones. With respect to the risk for breast cancer, heart disease, heart attack, and stroke, substantial scientific and medical evidence demonstrates that bioidentical hormones are safer and more efficacious forms of HRT than commonly used synthetic versions.”82
Given the preponderance of evidence, maturing women should feel confident that bioidentical hormone replacement, when appropriately prescribed, offers a safer and potentially even more effective alternative to conventional hormone replacement with non-bioidentical hormone drugs to help relieve menopausal symptoms and optimize long-term health. The addition of several proven nutrients to a bioidentical hormone regimen may help optimize estrogen metabolism and reduce cancer risk even further, offering an optimal, balanced approach to health maintenance. If you have any questions on the scientific content of this article, please call a Life Extension® Wellness Specialist at 1-866-864-3027 or visit www.lifeextension.com Acknowledgement: The Life Extension® would like to thank the following diverse group of experts in the scientific disciplines of allopathic medicine, nutrition, biochemistry, and integrative health care for their independent, peer-review of this position paper. John Boik, PhD James Cennamo, DO Mark L. Gordon, MD Steven Harris, MD Kent Holtorf, MD Richard Kratz, MD Peter Langsjoen, MD Erika Schwartz, MD Jonathan Wright, MD | ||
| References | ||
| 1. JAMA. 2002 Jul 17;288(3):321-33. 2. JAMA. 2004 Apr 14;291(14):1701-12. 3. Ann Intern Med. 2004 Jul 20;141(2):118-25. 4. https://www.health.harvard.edu/newsweek/ What-are-bioidentical-hormones.htm. 5. Climacteric. 2002 Sep;5(3):229-35. 6. J Steroid Biochem Mol Biol. 2005 Jul;96(2):95-108. 7. Breast Cancer Res Treat. 2001 Aug;68(3):187-98. 8. J Clin Endocrinol Metab. 1999 Dec;84(12):4559-65. 9. Cancer Res. 1992 Dec 1;52(23):6539-46. 10. Mol Cell Endocrinol. 1994 Jun;102(1-2):45-52. 11. Cancer Res. 1990 Dec 15;50(24):7858-62. 12. Biochem Biophys Res Commun. 1987 Jun 15;145(2):706-11. 13. Br J Cancer. 1993 May;67(5):945-52. 14. Breast Cancer Res Treat. 2007 Jan;101(2):125-34. 15. Breast Cancer Res Treat. 1998 Apr;48(3):221-9. 16. Am J Obstet Gynecol. 1996 Jan;174(1 Pt 1):93-100. 17. Cancer Lett. 1986 Feb;30(2):213-8. 18. Fertil Steril. 1995 Apr;63(4):785-91. 19. Fertil Steril. 1998 May;69(5):963-9. 20. Climacteric. 2003 Sep;6(3):221-7. 21. Jpn J Cancer Res. 1985 Aug;76(8):699-704. 22. J Gynecol Obstet Biol Reprod (Paris). 1990;19(3):269-74. 23. J Steroid Biochem Mol Biol. 2000 Jun;73(3-4):171-81. 24. Breast Cancer Res Treat. 1986;8(3):179-88. 25. Int J Cancer. 2005;114:448–54. 26. JAMA. 2003 Jun 25;289(24):3243-53. 27. Cancer Causes Control. 2002 Nov;13(9):847-54. 28. Br J Cancer. 2005 Jun 6;92(11):2049-58. 29. Br J Cancer. 2005 Apr 11;92(7):1293-7. 30. Cancer Epidemiol Biomarkers Prev. 2002 Jul;11(7):593-600. 31. Int J Cancer. 2004 May 1;109(5):721-7. 32. Maturitas. 2004 Sep 24;49(1):44-50. 33. Int J Cancer. 1999 May 5;81(3):339-44. 34. JAMA. 2000 Aug 9;284(6):691-4. 35. J Natl Cancer Inst. 2000 Feb 16;92(4):328-32. 36. Am J Obstet Gynecol. 2004 Apr;190(4):1141-67. 37. Obstet Gynecol. 2002 Dec;100(6):1148-58. 38. JAMA. 2003 Jun 25;289(24):3254-63. 39. Lancet. 2003 Aug 9;362(9382):419-27. 40. Cancer Causes Control. 2002 Aug;13(6):583-90. 41. Lancet. 1997 Oct 11;350(9084):1047-59. 42. JAMA. 2000 Jan 26;283(4):485-91. 43. Am J Epidemiol. 1998;147:S45. 44. Cancer Causes Control. 1999 Aug;10(4):253-60. 45. JAMA. 2002 Feb 13;287(6):734-41. 46. Steroids. 2000 Oct;65(10-11):659-64. 47. J Clin Endocrinol Metab. 2001 Jan;86(1):16-23. 48. Acta Obstet Gynecol Scand. 2003 Jul;82(7):335-44. 49. Breast Cancer Res Treat. 2008 Jan;107(1):103-11. 50. Cancer Detect Prev. 1999;23(4):290-6. 51. Int J Cancer. 2004 Nov 1;112(2):312-8. 52. Am J Epidemiol. 1981 Aug;114(2):209-17. 53. Cancer Epidemiol Biomarkers Prev. 2002 Apr;11(4):361-8. 54. Eur J Cancer. 1994;30A(4):445-8. 55. Br J Cancer. 1996 Jun;73(12):1552-5. 56. Yakushigaku Zasshi. 2001;36(1):70-5. 57. Fertil Steril. 1999 Sep;72(3):389-97. 58. Exp Clin Psychopharmacol. 2007 Oct;15(5):427-44. 59. Climacteric. 2008 Aug;11(4):273-9. 60. www.karger.com/gazette/66/mcewen/art_05.htm. 61. Endocrinology. 2004 Dec;145(12):5745-56. 62. Fertil Steril. 2000 Mar;73(3):516-21. 63. Hum Reprod Update. 1999 Jul-Aug;5(4):365-72. 64. Best Pract Res Clin Obstet Gynaecol. 2008 Apr;22(2):391-405. 65. Menopause. 2005 Mar;12(2):232-7. 66. Mol Endocrinol. 1997 Nov;11(12):1868-78. 67. Cancer. 1989 May 1;63(9):1685-92. 68. Cancer Res. 2004 Jan 1;64(1):423-8. 69. Science. 1997 Sep 5;277(5331):1508-10. 70. Proc Natl Acad Sci USA. 1996 Jun 11;93(12):5925-30. 71. J Steroid Biochem. 1986 Jan;24(1):77-83. 72. Recent Prog Horm Res. 2000;55:163-93. 73. Physiol Rev. 2001 Oct;81(4):1535-65. 74. Oncogene. 2005 Oct 6;24(44):6605-16. 75. Endocr Relat Cancer. 2004 Sep;11(3):537-51. 76. Breast. 2002 Aug;11(4):295-300. 77. Chem Biol. 2001 May;8(5):427-36. 78. Oncogene. 2000 Oct 12;19(43):4970-8. 79. Proc Natl Acad Sci USA. 2000 Jan 4;97(1):337-42. 80. Endocrinology. 2006 Sep;147(9):4132-50. 81. Proc Natl Acad Sci USA. 2002 Jun 25;99(13):8562-7. 82. Postgrad Med. 2009 Jan;121(1):73-85. 83. Int J Cancer. 2004 Oct 20;112(1):130-4. 84. Sitieri PK, Sholtz PI, Cirillo PM, et al. Prospective study of estrogens during pregnancy and the risk of breast cancer. Unpublished study performed in at the Public Health Institute in Oakland, California, and funded by the US Army Medical Research and Material Command under DAMD 17- 99-1-9358. 85. N Engl J Med. 1975 Dec 4;293(23):1167-70. 86. Am J Obstet Gynecol. 1977 Mar 15;127(6):572-80. 87. Am J Epidemiol. 2009 Jul 1;170(1):12-23. 88. Lancet. 1999 May 29;353(9167):1824-8. 89. Eur J Obstet Gynecol Reprod Biol. 1995 Sep;62(1):101-6. 90. Fertil Steril. 2003 Jan;79(1):221-2. 91. Menopause. 2003 Jul;10(4):373-4. 92. Menopause. 2003 Jul-Aug;10(4):374-7. 93. Maturitas. 2005 Oct 16;52(2):111-8. 94. J Am Coll Cardiol. 2003 Apr 16;41(8):1358-63. 95. Arterioscler Thromb Vasc Biol. 2004 Oct;24(10):e164-7. 96. Climacteric. 2003 Mar;6(1):45-52. 97. MedGenMed. 2006;8(3):40. 98. Climacteric. 2004 Dec;7(4):347-56. 99. Fertil Steril. 1993 May;59(5):992-7. 100. Maturitas. 1994 Aug;19(2):103-15. 101. J Steroid Biochem Mol Biol. 2007 Mar;103(3-5):708-11. 102. Cancer Res. 2005 Jun 15;65(12):5470-9. 103. Am J Public Health. 2006 Feb;96(2):252-61. 104. J Nutr. 2004 May;134(5):1134-8. 105. Nutr Cancer. 2002;42(1):1-9. 106. Cancer Res. 1999 Aug 15;59(16):3991-7. 107. Cancer Epidemiol Biomarkers Prev. 2000 May;9(5):477-85. 108. Mutat Res. 2007 May;635(2-3):90-104. 109. Cancer Res. 2005 Sep 15;65(18):8548-57. 110. Cancer Epidemiol Biomarkers Prev. 2000 Aug;9(8):773-9. 111. J Natl Cancer Inst. 1997 May 21;89(10):718-23. 112. J Cell Biochem.Suppl. 1997;28-29:111-6. 113. Cancer Epidemiol Biomarkers Prev. 2007 Mar;16(3):538-45. 114. Am J Clin Nutr. 1999 Sep;70(3 Suppl):439S-50S. 115. J Natl Cancer Inst. 2003 Jun 18;95(12):906-13. 116. Cancer Epidemiol Biomarkers Prev. 2003 Jul;12(7):665-8. 117. Lancet. 1991 May 18;337(8751):1197-200. 118. Cancer Lett. 1990 Jan;49(1):51-7. 119. Isr J Med Sci. 1995 Feb;31(2-3):101-5. 120. Carcinogenesis. 1986 Sep;7(9):1463-6. 121. Anticancer Res. 1995 May;15(3):805-10. 122. Int J Cancer. 2004 Sep 1;111(3):440-3. 123. Eur J Cancer. 2004 Jan;40(1):84-9. 124. Br J Cancer. 2007 Apr 10;96(7):1139-46. 125. Cancer Epidemiol Biomarkers Prev. 2007 Jul;16(7):1443-8. 126. Simone CB. Cancer and Nutrition. Lawrenceville, NJ: Princeton Institute; 2005. 127. Am J Clin Nutr. 2007 Jun;85(6):1586-91. 128. Nutr Rev. 2008 Oct;66(10 Suppl 2):S116-24. 129. N Engl J Med. 2000 Nov 23;343(21):1566-8. 130. Recent Results Cancer Res. 2003;164:99-110. 131. J Am Coll Cardiol. 2000 Dec;36(7):2154-9. 132. Circulation. 2007 Feb 20;115(7):840-5. 133. Arterioscler Thromb Vasc Biol. 1998 Jul;18(7):1164-71. 134. Circulation. 1996 Nov 1;94(9):2221-7. 135. Arterioscler Thromb Vasc Biol. 1997 Jan;17(1):217-21. 136. Endocrinology. 1997 Aug;138(8):3330-9. 137. Cardiovasc Pathol. 2000 Nov;9(6):317-22. 138. Arteriosclerosis. 1990 Nov;10(6):1051-7. 139. J Intern Med. 2008;263(3):256-73. 140. Maturitas. 1990 Jun;12(2):89-97. 141. JAMA. 1995 Jan 18;273(3):199-208. 142. Eur J Clin Invest. 1983 Dec;13(6):447-53. 143. Fertil Steril. 1981 Feb;35(2):172-9. 144. Clin Pharmacol Ther. 1980 Nov;28(5):602-4. 145. N Engl J Med. 1981 Mar 5;304(10):560-3. 146. Acta Obstet Gynecol Scand Suppl. 1984;127:1-37. 147. Am J Obstet Gynecol. 1985 Mar 15;151(6):746-50. 148. Am J Obstet Gynecol. 1987 Jan;156(1):66-71. 149. Hum Reprod. 2000 May;15(5):1028-36. 150. Nippon Ronen Igakkai Zasshi. 1996 May;33(5):353-9. 151. Life Sci. 2002 May 24;71(1):31-42. 152. J Womens Health Gend Based Med. 2000 May;9(4):381-7. 153. Menopause. 2002 Jul;9(4):253-63. 154. Obstet Gynecol. 1989 Apr;73(4):606-12. 155. Obstet Gynecol. 2002 Nov;100(5 Pt 1):853-63. 156. Menopause. 2001 Jan;8(1):10-6. 157. Clin Ther. 2001 Jul;23(7):1099-115. 158. JAMA. 1978 Apr 21;239(16):1638-41. 159. Horm Metab Res. 1987 Nov;19(11):579-84. 160. J Obstet Gynaecol Res. 1996 Jun;22(3):259-65. 161. Nippon Sanka Fujinka Gakkai Zasshi. 1996 Feb;48(2):83-8. 162. J Bone Miner Metab. 1998; 16:21-6. 163. Menopause. 2004 Jan;11(1):49-56. 164. N Engl J Med. 1993 Sep 9;329(11):753-6. 165. Eur J Obstet Gynecol Reprod Biol. 1993 Sep;51(1):29-33. 166. Orv Hetil. 1995 Feb 12;136(7):343-5. 167. Maturitas. 2001 Sep 28;39(3):253-7. 168. J Cosmet Dermatol. 2006 Mar;5(1):3-8. 169. Menopause Int. 2007 Jun;13(2):60-4. 170. Clin Interv Aging. 2007;2(3):283-97. 171. Exp Dermatol. 2002 Dec;11(6):487-502. 172. Eur J Obstet Gynecol Reprod Biol. 2007 Feb;130(2):202-5. 173. Int J Dermatol. 1996 Sep;35(9):669-74. 174. Br Med J (Clin Res Ed). 1983 Nov 5;287(6402):1337-8. 175. Arch Dermatol. 1997 Mar;133(3):339-42. 176. Altern Med Rev. 1998 Apr;3(2):101-13. 177. Maturitas. 1994 Nov;20(1):25-30. 178. Climacteric. 2007 Aug;10(4):289-97. 179. Essex Testing Clinic, Inc. Data on file. 180. Endocr Metab Immune Disord Drug Targets. 2009 Mar;9(1):29-37. 181. J Sex Med. 2008 Oct;5(10):2282-90. 182. Gynecol Endocrinol. 2009 Jan;25(1):12-20. 183. Rev Med Suisse. 2007 Mar 28;3(104):792-6. 184. N Engl J Med. 2008 Nov 6;359(19):2005-17. 185. Am J Clin Nutr. 2009 May;89(5):1459-67. 186. Metabolism. 2008 Jun;57(6):838-44. 187. J Clin Endocrinol Metab. 1990 Feb;70(2):473-9. 188. Obes Rev. 2004 Nov;5(4):197-216. 189. Maturitas. 2008 May 20;60(1):10-8. 190. Am J Obstet Gynecol. 1998 Jan;178(1 Pt 1):101-7. 191. Acta Diabetol. 2003 Oct;40 Suppl 1:S191-5. 192. Eur J Contracept Reprod Health Care. 2000 Dec;5 Suppl 3:9-16. 193. Cancer Lett. 1997 Mar 19;114(1-2):169-70. 194. J Endocrinol. 1996 Sep;150 SupplS259-65. 195. Cell Cycle. 2008 Apr 1;7(7):917-24. 196. Cancer Prev Res (Phila Pa). 2009 Jun;2(6):598-604. 197. Mol Cancer Ther. 2007 Apr;6(4):1433-9. 198. Cancer Res. 2007 Dec 15;67(24):11840-7. 199. Carcinogenesis. 2008 Jan;29(1):93-9. 200. Am J Clin Nutr. 2008 Jun;87(6):1952-8. 201. Am J Clin Nutr. 2009 Apr;89(4):1132-7. 202. Nutr Cancer. 2004;50(2):161-7. 203. Lancet. 2005 Oct 29;366(9496):1558-60. 204. Epidemiology. 2000 Nov;11(6):635-40. 205. Otolaryngol Head Neck Surg. 2001 Mar;124(3):241-7. 206. Cancer Epidemiol Biomarkers Prev. 1997 Jul;6(7):505-9. 207. Epidemiology. 2006 Jan;17(1):80-8. 208. Steroids. 2003 Jan;68(1):65-72. 209. Cancer Res. 1999 Mar 15;59(6):1244-51. 210. Cancer Res. 1994 Nov 15;54(22):5848-55. 211. Jpn J Cancer Res. 1995 Feb;86(2):146-54. 212. Cancer Causes Control. 1998 Dec;9(6):553-7. 213. JAMA. 2005 Sep 28;294(12):1493-504. 214. Am J Epidemiol. 2007 Oct 15;166(8):924-31. 215. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2005 Apr;27(2):258-61. 216. J Nutr. 2002 Feb;132(2):276-82. 217. Nutr J. 2005;430. 218. J Nutr. 1995 Mar;125(3 Suppl):777S-83S. 219. J Am Coll Nutr. 2001 Oct;20(5 Suppl):354S-62S. 220. J Natl Cancer Inst. 2003 Aug 6;95(15):1158-64. 221. Cancer Epidemiol Biomarkers Prev. 2005 Jan;14(1):81-90. 222. Asia Pac J Clin Nutr. 2006;15(1):21-9. 223. Int J Cancer. 2007 Jul 15;121(2):377-85. 224. Int J Cancer. 2002 Mar 1;98(1):78-83. 225. www.garfield.library.upenn.edu/histcomp/kritchevsky-d_auth-citing/node/7082.html 226. Biochem Med Metab Biol. 1990 Apr;43(2):83-92. 227. Cancer Detect Prev. 1997;21(2):178-90. 228. Altern Med Rev. 2002 Aug;7(4):336-9. 229. Slaga TJ, Quilici-Timmcke J. D-Glucarate: A Nutrient Against Cancer. Columbus, Ohio: McGraw-Hill; 1999. 230. Clin Cancer Res. 2005 May 15;11(10):3828-35. 231. Cancer Biol Ther. 2007 Dec;6(12):1938-43. 232. Cancer Lett. 2007 Jan 8;245(1-2):232-41. 233. Breast Cancer Res Treat. 2008 Feb;107(3):359-69. 234. J Exp Ther Oncol. 2002 Nov;2(6):350-9. 235. Cancer Detect Prev. 2007;31(6):499-504. 236. Ann NY Acad Sci. 2007 Jan;1095:428-40. 237. http://www.fasebj.org/cgi/content/meeting_abstract/22/1_MeetingAbstracts/1164.3. 238. Int J Cancer. 2003 Sep 10;106(4):574-9.
|
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun