Life Extension Magazine®

Misconceptions About Atherosclerosis
Cardiovascular disease causes one of every three deaths in the United States. Most heart attacks and strokes are caused by atherosclerosis. Because mainstream doctors only treat one or two of the multifactorial causes of this disease, heart attacks remain the leading cause of death. Reduce your risk by taking steps to manage and eliminate all 17 proven causes of arterial disease.
Scientifically reviewed by Dr. Gary Gonzalez, MD, in October 2024. Written by: William Faloon.
Atherosclerosis is the underlying cause of most heart attacks and strokes, yet doctors remain confused as to how this artery-blocking process occurs.
Most cardiologists overlook specific mechanisms that inflict arterial wall damage and the ensuing progression to occlusive atherosclerotic disease. The result is that only a few of the factors that accelerate arterial blockage (such as elevated LDL) are addressed in today’s clinical setting.
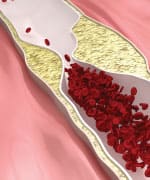
Doctors think of an atherosclerotic lesion as a “clog” consisting of fat, cholesterol, and platelets that have accumulated on an inner arterial wall. As a result, they tell their patients to eat less fat, take a statin drug (if cholesterol levels are high), and use a baby aspirin to prevent arterial platelet aggregation. The problem with these approaches is that while they may postpone a heart attack or stroke, they fail to correct the underlying pathologies that cause atherosclerotic lesions to form and progress.
If people are to live long lives free of the ravages of atherosclerosis, these lethal misconceptions must be cleared up. Otherwise, there will be an epidemic of aging people receiving coronary stents, undergoing bypass surgeries, and dropping dead from sudden heart attacks.Why Arteries Clog as We Age
The aging process damages blood vessels, even when conventional risk factors such as cholesterol and blood pressure are within normal ranges.
For over 40 years, the standard treatment for coronary atherosclerosis has been to bypass the blocked arteries. Recuperation from this procedure can take months, and some patients are afflicted with lifetime impairments such as chronic inflammation, memory loss, and depression.1-11
Stenting open narrowed coronary arteries has become prevalent over the past decade, but this procedure is not a cure for underlying systemic endothelial dysfunction and atherosclerosis.
A review of the scientific literature reveals that atherosclerosis is associated with high blood levels of homocysteine,12-14 fibrinogen,15-18 C-reactive protein,12,15,19-26 glucose,27,28 cholesterol,29-32 insulin,33-36 iron,37-40 LDL,41-44 and triglycerides,45-48 along with low levels of HDL49-52 and testosterone (in men).53-58 Optimizing blood levels of these substances can dramatically reduce heart attack and stroke risk.
Despite thousands of studies validating that atherosclerosis is a multifactorial process, today’s doctors often prescribe a statin drug as the sole therapy to prevent and treat coronary atherosclerosis. Mainstream cardiologists fail to appreciate that coronary atherosclerosis is a sign of systemic arterial dysfunction requiring aggressive therapy to correct.
Anatomy of the Artery

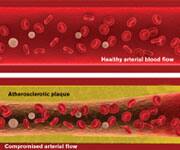
Arteries are the blood vessels that bear the full force of each heartbeat. Most people think of arteries as flexible tubes whose only function is to carry blood that flows continuously throughout the body. In fact, arteries are dynamic, functioning muscular structures that, when healthy, expand and contract to facilitate circulation and maintain optimal blood pressure.
The outer layer of the artery comprises mostly connective tissue and provides structural containment for the two layers beneath. The middle area comprises elastic smooth muscle that provides the contractile strength to make possible the artery’s expansion and contraction with each heartbeat. The inner layer, known as the endothelium, comprises a thin area of endothelial cells whose integrity is crucial if atherosclerosis is to be prevented.
Poor health habits and normal aging result in endothelial dysfunction, a process in which the endothelium boundary is broken, arterial flexibility is diminished, abnormal platelet aggregation occurs, and atherosclerotic lesions form in response to arterial wall (endothelium) injuries.
How Do Most Heart Attacks and Strokes Occur?
The two prime factors involved in occlusive arterial disease are abnormal platelet aggregation and endothelial dysfunction. When the endothelium is not functioning properly, our platelets (blood-clotting cells) become dangerously over-activated. This can cause a sudden arterial blood clot, or contribute to progression of atherosclerosis by stimulating inflammation.
A primary mechanism involved in endothelial dysfunction is the depletion of nitric oxide, often caused from the oxidation of LDL and other blood components. Nitric oxide is produced by endothelial cells. It regulates vascular elasticity, maintains cardiac contraction, prevents vessel injury, and helps protect against atherosclerosis.59-62
As humans age, endothelial function becomes altered. Due to a variety of insults, a depletion of nitric oxide occurs in the endothelium. One consequence of nitric oxide depletion is the inability of arteries to expand and contract with youthful elasticity. The continual stiffening and occlusion of aged arteries is the number one health risk that people in Western societies face.63-68 In order to maintain healthy arterial dilation, the endothelium has to manufacture enough nitric oxide. Impairment in nitric oxide release by the aging endothelium causes arterial dysfunction.69,70
Therapies used by today’s mainstream cardiologists (aspirin, statin, and certain anti-hypertensive drugs) have a beneficial effect on the endothelium, but they may only postpone a serious vascular event. If a person lives long enough, the chronic depletion of endothelial nitric oxide results in impairment of arterial function and progressive restriction of blood flow to vital parts of the body.
What You Need to Know
 |
Guard Against Lethal Medical Misconceptions
- Doctors think of an atherosclerotic lesion as a “clog” consisting of fat, cholesterol, and platelets that have accumulated on an inner arterial wall.
- Despite thousands of studies validating that atherosclerosis is a multifactorial process, today’s doctors often prescribe a statin drug as the sole therapy to prevent and treat coronary atherosclerosis.
- Stenting open narrowed coronary arteries has become prevalent over the past decade, but this procedure is not a cure for underlying systemic endothelial dysfunction and atherosclerosis.
- The aging process damages blood vessels, even when conventional risk factors such as cholesterol and blood pressure are within normal ranges.
- A review of the scientific literature reveals that atherosclerosis is associated with high blood levels of homocysteine, fibrinogen, C-reactive protein, glucose, cholesterol, insulin, iron, LDL, and triglycerides, along with low levels of HDL and testosterone (in men).
- Poor health habits and normal aging result in endothelial dysfunction, a process in which the endothelium boundary is broken, arterial flexibility is diminished, abnormal platelet aggregation occurs, and athero-sclerotic lesions form in response to arterial wall (endothelium) injuries.
- A primary mechanism involved in endothelial dysfunction is the depletion of nitric oxide, often caused from the oxidation of LDL and other blood components.
- Annual blood testing is critical to identifying one’s individual risk factors.
Summary
Endothelial cells line the arteries, veins, arterioles, and capillaries of the vascular system. Doctors used to view the endothelium as a relatively inert structure that played no active role in vascular function. Starting around 20 years ago, research has shown that the endothelium is dynamic and participates in vital aspects of arterial structure and function.74
Over the years, Life Extension® has reported on advances related to protecting the endothelium against age-related deterioration, such as the remarkable ability of pomegranate to reverse clinical measurements of systemic atherosclerosis (in both carotid and coronary arteries).75-81
A typical 50-year-old human can postpone a major cardiovascular event by following relatively simple steps, such as eating healthy and taking a low-dose statin drug if LDL is over 100 mg/dL. As that same person ages, however, multiple processes involved in endothelial dysfunction too often manifest in the form of a vascular-related disorder.
Endothelial cells that line blood vessels are crucial to maintaining vascular integrity. Endothelial dysfunction is a critical factor in the initiation and progression of cardiovascular disease,82-84 yet mainstream doctors continue to ignore this dominant underlying cause of arterial occlusion. Pomegranate extracts protect against endothelial dysfunction via several well-defined mechanisms, including protection of vital endothelial nitric oxide.85-87
Atherosclerosis remains the number-one cause of death and disability in the United States.88 The graphic on the next page shows 17 independent risk factors of atherosclerosis, with low EPA/DHA blood levels being only one of the elements that must be controlled if heart attack and ischemic stroke are to be averted.
Annual blood testing is critical to identifying one’s individual risk factors. Modest-dose fish oil alone will not reverse the endothelial dysfunction that exists in aging humans with preexisting atherosclerosis.
To read specifically how atherosclerosis initiates and progresses, refer to the next article.If you have any questions on the scientific content of this article, please call a Life Extension® Health Advisor at 1-866-864-3027.
Why Some Elderly People Need More Than a Statin Drug
 |
Did you know that popular “statin” drugs used to reduce LDL and cholesterol often lose their ability to protect against vascular disease as people age?71-73 The reason is simple. Aging arteries are subjected to more destructive forces than blood vessels of young people.
Statins have shown beneficial effects to the endothelium in addition to reducing cholesterol and LDL. As we age, however, we must go beyond basic therapies (such as statin drugs) that may have protected us in younger years.
Prevention of the epidemic of stroke and heart disease in the elderly requires that we aggressively counteract the underlying causes of endothelial dysfunction.
Some people require the proper dose of statin drug to control excess cholesterol-LDL, but all aging humans need to take assertive actions to protect their precious endothelium against the functional and structural distortions that lead to arterial occlusion.
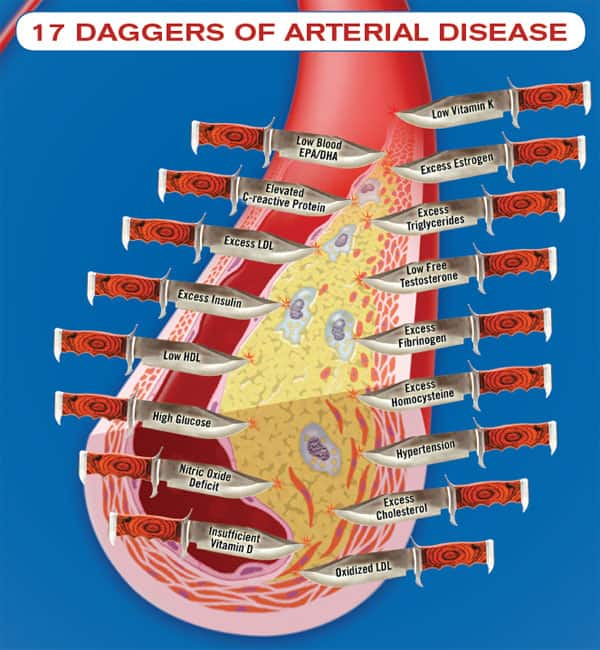
This image depicts daggers aimed at an artery occluded with atherosclerotic plaque. Any one of these “daggers” can initiate and propagate vascular disease. In the real world, aging humans suffer small pricks from the point of these daggers over a lifetime. The cumulative effect of these dagger pricks (risk factors) is arterial occlusion and, far too often, stroke or acute heart attack.
References
- Suksompong S, Prakanratrana U, Chumpathong S, Sriyoschati S, Pornvilawan S. Neuropsychological alterations after coronary artery bypass graft surgery. J Med Assoc Thai. 2002 Sep;85 Suppl 3:S910-6.
- Strauss B, Paulsen G, Strenge H, Graetz S, Regensburger D, Speidel H. Preoperative and late postoperative psychosocial state following coronary artery bypass surgery. Thorac Cardiovasc Surg. 1992 Apr;40(2):5964.
- Scholz M, Nowak P, Blaheta R, et al. Relocalization of endothelial cell betacatenin after coculture with activated neutrophils from patients undergoing cardiac surgery with cardiopulmonary bypass. Invest Surg. 2004 May-Jun;17(3):143-9.
- Dacey LJ, DeSimone J, Braxton JH, et al. Preoperative white blood cell count and mortality and morbidity after coronary artery bypass grafting. Ann Thorac Surg. 2003 Sep;76(3):760-4.
- Wei M, Kuukasjarvi P, Laurikka J, et al. Relation of cytokines to vasodilation after coronary artery bypass grafting. World J Surg. 2003 Oct;27(10):1093-8.
- Bergh C, Backstrom M, Jonsson H, Havinder L, Johnsson P. In the eye of both patient and spouse: memory is poor 1 to 2 years after coronary bypass and angioplasty. Ann Thorac Surg. 2002 Sep;74(3):689-93.
- Fearn SJ, Pole R, Wesnes K, Faragher EB, Hooper TL, McCollum CN. Cerebral injury during cardiopulmonary bypass: emboli impair memory. J Thorac Cardiovasc Surg. 2001 Jun;121(6):1150-60.
- Newman MF, Kirchner JL, Phillips-Bute B, et al. Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. N Engl J Med. 2001 Feb 8;344(6):395-402.
- Phillips Bute B, Mathew J, Blumenthal JA, et al. Female gender is associated with impaired quality of life 1 year after coronary artery bypass surgery. Psychosom Med. 2003 Nov-Dec;65(6):944-51.
- Rymaszewska J, Kiejna A. Depression and anxiety after coronary artery bypass grafting. Pol Merkuriusz Lek. 2003 Aug;15(86):193-5.
- Blumenthal JA, Lett HS, Babyak MA, et al. Depression as a risk factor for mortality after coronary artery bypass surgery. Lancet. 2003 Aug 23;362(9384):604-9.
- Jarosz A, Nowicka G. C-reactive protein and homocysteine as risk factors of atherosclerosis. Przegl Lek. 2008 65(6):268-72.
- Rasouli ML, Nasir K, Blumenthal RS, Park R, Aziz DC, Budoff MJ. Plasma homocysteine predicts progression of atherosclerosis. Atherosclerosis. 2005 Jul;181(1):159-65.
- Bots ML, Launer LJ, Lindemans J, Hofman A, Grobbee DE. Homocysteine, atherosclerosis and prevalent cardiovascular disease in the elderly: The Rotterdam Study. J Intern Med. 1997 Oct;242(4):339-47.
- Ridker PM, Stampfer MJ, Rifai N. Novel risk factors for systemic atherosclerosis: a comparison of C-reactive protein, fibrinogen, homocysteine, lipoprotein(a), and standard cholesterol screening as predictors of peripheral arterial disease. JAMA. 2001 May 16;285(19):2481-5.
- Maresca G, Di Blasio A, Marchioli R, Di Minno G. Measuring plasma fibrinogen to predict stroke and myocardial infarction: an update. Arterioscler Thromb Vasc Biol. 1999 Jun;19(6):1 368-77.
- Acevedo M, Foody JM, Pearce GL, Sprecher DL. Fibrinogen: associations with cardiovascular events in an outpatient clinic. Am Heart J. 2002 Feb;143(2):277-82.
- Thompson SG, Kienast J, Pyke SD, Haverkate F, van de Loo JC. Hemostatic factors and the risk of myocardial infarction or sudden death in patients with angina pectoris. N Engl J Med. 1995 Mar 9;332(10):635-41.
- Van Der Meer IM, De Maat MP, Hak AE, et al. C-reactive protein predicts progression of atherosclerosis measured at various sites in the arterial tree: The Rotterdam Study. Stroke. 2002 Dec;33(12):2750-5.
- Masood A, Jafar SS, Akram Z. Serum high sensitivity C-reactive protein levels and the severity of coronary atherosclerosis assessed by angiographic gensini score. J Pak Med Assoc. 2011 Apr;61(4):325-7.
- Agmon Y, Khandheria BK, Meissner I, et al. C-reactive protein and atherosclerosis of the thoracic aorta: a population-based transesophageal echocardiographic study. Arch Intern Med. 2004 Sep 13;164(16):1781-7.
- Choi EY, Yan RT, Fernandes VR, et al. High-sensitivity C-reactive protein as an independent predictor of progressive myocardial functional deterioration: the multiethnic study of atherosclerosis. Am Heart J. 2012 Aug;164(2):251-8.
- Piechota W, Piechota W. Correlation of high-sensitivity CRP concentration with the extent of coronary atherosclerosis in men with symptoms of ischemic heart disease. Pol Merkur Lekarski. 2005 May;18(107):511-5.
- Mendall MA, Strachan DP, Butland BK, et al. C-reactive protein: relation to total mortality, cardiovascular mortality and cardiovascular risk factors in men. Eur Heart J. 2000 Oct;21(19):1584-90.
- Ridker PM, Buring JE, Shih J, Matias M, Hennekens CH. Prospective study of C- reactive protein and the risk of future cardiovascular events among apparently healthy women. Circulation. 1998 Aug 25;98(8):731-3.
- Pasceri V, Willerson JT, Yeh ET. Direct proinflammatory effect of C-reactive protein on human endothelial cells. Circulation. 2000 Oct 31;102(18):2165-8.
- MacDonald-Wicks L, Gibson LZ, Godfrey DM, et al. Oxidized LDL in newly diagnosed type 2 diabetes mellitus and impaired glucose tolerance. Asia Pac J Clin Nutr. 2004 13(Suppl):S65.
- Ceriello A. Impaired glucose tolerance and cardiovascular disease: the possible role of post-prandial hyperglycemia. Am Heart J. 2004 May;147(5):803-7.
- Zulli A, Widdop RE, Hare DL, Buxton BF, Black MJ. High methionine and cholesterol diet abolishes endothelial relaxation. Arterioscler Thromb Vasc Biol. 2003 Aug 1;23(8):1358-63.
- Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med. 2002 Nov 14;347(20):1557-65.
- Guize L, Benetos A, Thomas F, Malmejac A, Ducimetiere P. Cholesterolemia and total, cardiovascular and cancer mortality. Study of a cohort of 220,000 people. Bull Acad Natl Med. 1998 182(3):631-47.
- Kashyap ML. Cholesterol and atherosclerosis: a contemporary perspective. Ann Acad Med Singapore. 1997 Jul; 26(4):517-23.
- Stout RW. The relationship of abnormal circulating insulin levels to atherosclerosis. Atherosclerosis. 1977 May;27(1):1-13.
- Bonora E, Kiechl S, Willeit J, et al. Insulin resistance as estimated by homeostasis model assessment predicts incident symptomatic cardiovascular disease in caucasian subjects from the general population: the Bruneck study. Diabetes Care. 2007 Feb;30(2):318-24.
- Takahashi F, Hasebe N, Kawashima E, et al. Hyperinsulinemia is an independent predictor for complex atherosclerotic lesion of thoracic aorta in non-diabetic patients. Atherosclerosis. 2006 Aug;187(2):336-42..
- Stochmal E, Szurkowska M, Czarnecka D, et al. Association of coronary atherosclerosis with insulin resistance in patients with impaired glucose tolerance. Acta Cardiol. 2005 Jun;60(3):325-31.
- Shah SV, Alam MG. Role of iron in atherosclerosis. Am J Kidney Dis. 2003 Mar;41(3 Suppl 1):S80-3.
- Kraml P, Potockova J, Koprivova H, et al. Ferritin, oxidative stress and coronary atherosclerosis. Vnitr Lek. 2004 Mar;50(3):197-202.
- Armaganijan D, Batlouni M. Serum ferritin levels and other indicators of organic iron as risk factors or markers in coronary artery disease. Rev Port Cardiol. 2003 Feb;22(2):185-95; discussion 197-201.
- Minqin R, Watt F, Huat BT, Halliwell B. Correlation of iron and zinc levels with lesion depth in newly formed atherosclerotic lesions. Free Radic Biol Med. 2003 Mar 15;34(6):746-52.
- Nissen SE, Tuzcu EM, Schoenhagen P, et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. JAMA. 2004 Mar 3;291(9):1071-80.
- Reed DM, Strong JP, Resch J, Hayashi T. Serum lipids and lipoproteins as predictors of atherosclerosis. An autopsy study. Arteriosclerosis. 1989 Jul-Aug;9(4):560-4.
- Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med. 2002 Nov 14;347(20):1557-65.
- Montalcini T, Gorgone G, Federico D, et al. Association of LDL cholesterol with carotid atherosclerosis in menopausal women affected by the metabolic syndrome. Nutr Metab Cardiovasc Dis. 2005 Oct;15(5):368-72.
- Nordestgaard BG, Benn M, Schnohr P, Tybjaerg-Hansen A. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA. 2007 Jul 18;298(3):299-308.
- Welin L, Eriksson H, Larsson B, et al Triglycerides, a major coronary risk factor in elderly men. A study of men born in 1913. Eur Heart J. 1991 Jun;12(6):700-4.
- Carlson LA, Bottiger LE, Ahfeldt PE. Risk factors for myocardial infarction in the Stockholm prospective study. A 14-year fol- low-up focusing on the role of plasma triglycerides and cholesterol. Acta Med Scand. 1979 206(5):351-60.
- Drexel H, Amann FW, Beran J, et al. Plasma triglycerides and three lipoprotein cholesterol fractions are independent predictors of the extent of coronary atherosclerosis. Circulation. 1994 Nov;90(5):2230-5
- Viles-Gonzalez JF, Fuster V, Corti R, Badimon JJ. Emerging importance of HDL cholesterol in developing high-risk coronary plaques in acute coronary syndromes. Curr Opin Cardiol. 2003 Jul;18(4):286-94.
- Spieker LE, Sudano I, Hurlimann D, et al. High-density lipoprotein restores endothelial function in hypercholesterolemic men. Circulation. 2002 Mar 26;105(12):1399-402.
- Phillips GB, Pinkernell BH, Jing TY. Are major risk factors for myocardial infarction the major predictors of degree of coronary artery disease in men? Metabolism. 2004 Mar;53(3):324-9.
- Toikka JO, Ahotupa M, Viikari JS, et al. Constantly low HDL-cholesterol concentration relates to endothelial dysfunction and increased in vivo LDL-oxidation in healthy young men. Atherosclerosis. 1999 Nov 1;147(1):133-8.
- Dunajska K, Milewicz A, Szymczak J, et al. Evaluation of sex hormone levels and some metabolic factors in men with coronary atherosclerosis. Aging Male. 2004 Sep;7(3):197-204.
- Hak AE, Witteman JC, de Jong FH, Geerlings MI, Hofman A, Pols HA. Low levels of endogenous androgens increase the risk of atherosclerosis in elderly men: The Rotterdam study. J Clin Endocrinol Metab. 2002 Aug;87(8):3632-9.
- Channer KS, Jones TH. Cardiovascular effects of testosterone: implications of the “male menopause”? Heart. 2003 Feb;89(2):121-2.
- English KM, Steeds RP, Jones TH, Diver MJ, Channer KS. Low-dose transdermal testosterone therapy improves angina threshold in men with chronic stable angina: A randomized, double-blind, placebo- controlled study. Circulation. 2000 Oct 17;102(16):1906-11.
- Jones RD, Nettleship JE, Kapoor D, Jones HT, Channer KS. Testosterone and atherosclerosis in aging men: purported association and clinical implications. Am J Cardiovasc Drugs. 2005 5(3):141-54.
- English KM, Mandour O, Steeds RP, et al. Men with coronary artery disease have lower levels of androgens than men with normal coronary angiograms. Eur Heart J. 2000 Jun;21(11):890-4.
- Rubio AR, Morales-Segura MA. Nitric oxide, an iceberg in cardiovascular physiology: far beyond vessel tone control. Arch Med Res. 2004 Jan-Feb;35(1):1-11.
- Shaw CA, Taylor EL, Megson IL, Rossi AG. Nitric oxide and the resolution of inflammation: implications for atherosclerosis. Mem Inst Oswaldo Cruz. 2005 Mar;100 Suppl 1:67-71.
- Shaul PW. Endothelial nitric oxide synthase, caveolae and the development of atherosclerosis. J Physiol. 2003 Feb 15;547(Pt 1):21-33.
- Takimoto E, Champion HC, Li M, Ren S, et al. Oxidant stress from nitric oxide synthase-3 uncoupling stimulates cardiac pathologic remodeling from chronic pressure load. J Clin Invest. 2005 May;115(5):1221-31.
- Aikawa K, Saitoh S, Muto M, et al. Effects of antioxidants on coronary microvascular spasm induced by epicardial coronary artery endothelial injury in pigs. Coron Artery Dis. 2004 Feb;15(1):21-30.
- Angdin M, Settergren G, Starkopf J, Zilmer M, Zilmer K, Vaage J. Protective effect of antioxidants on pulmonary endothelial function after cardiopulmonary bypass. J Cardiothorac Vasc Anesth. 2003 Jun;17(3):314-20.
- Meydani M. Dietary antioxidants modulation of aging and immune-endothelial cell interaction. Mech Aging Dev. 1999 Nov;111(2-3):123-32.
- Schubert SY, Neeman I, Resnick N. A novel mechanism for the inhibition of NF-kappaB activation in vascular endothelial cells by natural antioxidants. FASEB J. 2002 Dec;16(14):1931-3.
- Schulz E, Anter E, Keaney JF Jr. Oxidative stress, antioxidants, and endothelial function. Curr Med Chem. 2004 May;11(9): 1093-104.
- Taddei S, Virdis A, Ghiadoni L, et al. Age-related reduction of NO availability and oxidative stress in humans. Hypertension. 2001 Aug;38(2):274-9.
- Rubio AR, Morales-Segura MA. Nitric oxide, an iceberg in cardiovascular physiology: far beyond vessel tone control. Arch Med Res. 2004 Jan-Feb;35(1):1-11.
- Sugawara J, Komine H, Hayashi K, et al. Effect of systemic nitric oxide synthase inhibition on arterial stiffness in humans. Hypertens Res. 2007 May;30(5):411-5.
- Mungall MM, Gaw A. Statin therapy in the elderly. Curr Opin Lipidol. 2004 Aug;15(4):453-7.
- ten Dam VH, Box FM, de Craen AJ, et al. Lack of effect of pravastatin on cerebral blood flow or parenchymal volume loss in elderly at risk for vascular disease. Stroke. 2005 Aug;36(8):1633-6.
- Weverling-Rijnsburger AW, Blauw GJ, Meinders AE. Effect of atorvastatin on impaired vascular function in healthy old men. J Clin Pharm Ther. 2004 Apr;29(2):157-64.
- Rubanyi GM. The role of endothelium in cardiovascular homeostasis and diseases. J Cardiovasc Pharmacol. 1993 22 Suppl 4:S1-14.
- Aviram M, Rosenblat M, Gaitini D, et al. Pomegranate juice consumption for 3 years by patients with carotid artery stenosis reduces common carotid intima-media thickness, blood pressure and LDL oxidation. Clin Nutr. 2004 Jun;23(3):423-33.
- Kaplan M, Hayek T, Raz A, et al. Pomegranate juice supplementation to atherosclerotic mice reduces macrophage lipid peroxidation, cellular cholesterol accumulation and development of atherosclerosis. J Nutr. 2001 Aug;131(8):2082-9.
- Sumner MD, Elliott-Eller M, Weidner G, et al. Effects of pomegranate juice consumption on myocardial perfusion in patients with coronary heart disease. Am J Cardiol. 2005 Sep 15;96(6): 810-4.
- Aviram M, Dornfeld L, Kaplan M, et al. Pomegranate juice flavonoids inhibit low-density lipoprotein oxidation and cardiovascular diseases: studies in atherosclerotic mice and in humans. Drugs Exp Clin Res. 2002 28(2-3):49-62.
- Rosenblat M, Volkova N, Coleman R, et al. Pomegranate byproduct administration to apolipoprotein e-deficient mice attenuates atherosclerosis development as a result of decreased macrophage oxidative stress and reduced cellular uptake of oxidized low-density lipoprotein. J Agric Food Chem. 2006 Mar 8;54(5):1928-35.
- de Nigris F, Williams-Ignarro S, Sica V, et al. Effects of a pomegranate fruit extract rich in punicalagin on oxidation-sensitive genes and eNOS activity at sites of perturbed shear stress and atherogenesis. Cardiovasc Res. 2007 Jan 15;73(2):414-23.
- Aviram M, Hardak E, Vaya J, et al. Human serum paraoxonases (PON1) Q and R selectively decrease lipid peroxides in human coronary and carotid atherosclerotic lesions: PON1 esterase and peroxidase-like activities. Circulation. 2000 May 30;101(21): 2510-7.
- Ruilope LM, Redón J, Schmieder R. Cardiovascular risk reduction by reversing endothelial dysfunction: ARBs, ACE inhibitors, or both? Expectations from the ONTARGET Trial Programme. Vasc Health Risk Manag. 2007;3(1):1-9.
- Kinlay S, Ganz P. Role of endothelial dysfunction in coronary artery disease and implications for therapy. Am J Cardiol. 1997 Nov;80(9A):11I-16I.
- Zeiher AM, Drexler H, Wollschlager H, et al. Endothelial dysfunction of the coronary microvasculature is associated with coronary blood flow regulation in patients with early atherosclerosis. Circulation.1991 Nov;84(5):1984-92.
- de Nigris F, Williams-Ignarro S, Botti C, Sica V, Ignarro LJ, Napoli C. Pomegranate juice reduces oxidized low-density lipoprotein downregulation of endothelial nitric oxide synthase in human coronary endothelial cells. Nitric Oxide. 2006 Nov;15(3):259-63.
- Ignarro LJ, Byrns RE, Sumi D, de Nigris F, Napoli C. Pomegranate juice protects nitric oxide against oxidative destruction and enhances the biological actions of nitric oxide. Nitric Oxide. 2006 Sep;15(2):93-102.
- de Nigris F, Williams-Ignarro S, Lerman LO, et al. Beneficial effects of pomegranate juice on oxidation-sensitive genes and endothelial nitric oxide synthase activity at sites of perturbed shear stress. Proc Natl Acad Sci U S A. 2005 Mar 29;102(13):4896-901.
- Available at: http://www.cdc.gov/nchs/fastats/lcod.htm. Accessed December 21, 2012.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun