
Carpal Tunnel Syndrome
Carpal Tunnel Syndrome
Last Section Update: 05/2026
1 Overview
Summary and Quick Facts for Carpal Tunnel Syndrome
- A significant portion of the population will be affected by carpal tunnel syndrome (CTS) at some point in time, with estimates of lifetime prevalence ranging from 3-20%.
- In this protocol you will learn about the causes of CTS and how this condition is conventionally diagnosed and treated. A number of natural approaches that target some of the pathological mechanisms underlying CTS will be reviewed, as well.
- Surgical release of the transverse carpal ligament is a common method of relieving moderate to severe CTS, with over 500,000 procedures performed annually in the United States. Several integrative interventions such as B vitamins (especially B6), alpha-lipoic acid, omega-3 fatty acids, curcumin and the enzyme serratiopeptidase may also be helpful in easing symptoms.
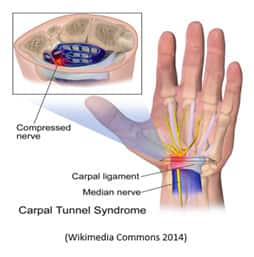
Carpal tunnel syndrome (CTS) is a relatively common disorder characterized by pain, tingling, numbness, or changes in sensation in the hands, wrists, or fingers. CTS results from irritation or compression of the median nerve, which travels from the wrist into the hand through a canal called the carpal tunnel.
Several integrative interventions, including B vitamins and acetyl-L-carnitine, may decrease the pain caused by CTS and improve hand function.
Causes and Risk Factors for CTS
- Repetitive use and trauma, including occupations that use jackhammers, chainsaws, and assembly line work. Studies on links between prolonged computer keyboard or mouse use and CTS have been inconclusive.
- Obesity
- Diabetes and metabolic syndrome
- Menopause, pregnancy and female hormones, as the age of peak incidence is 40‒60 years old
Symptoms of CTS
- Pain, numbness, and tingling in the wrist and first three fingers of the affected hand
- Forearm pain may occur
- Hand or wrist weakness may also be present
Diagnosis of CTS
- Positive Tinel’s sign; a tingling sensation when tapping on the carpal tunnel
- Positive Phalen’s maneuver; numbness and tingling when wrist is flexed
- Nerve conduction tests to detect delayed median nerve conduction rates
- Ultrasound of the wrist joint, carpal tunnel, and median nerve
Conventional Treatment for CTS
- Injectable corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs), and lidocaine patches are considered conservative treatment for mild-to-moderate CTS
- Carpal tunnel release surgery when conservative treatment fails
- Massage and manual manipulation techniques have improved CTS symptoms and splinting may be recommended
Novel and Emerging Strategies for CTS
- Sonographically guided percutaneous needle release may provide similar results to minimally invasive surgery with lower risk and recovery time
- Low-level laser therapy may improve various symptoms and be as effective as surgical treatment for mild-to-moderate CTS
- Microwave heat treatment, using microwaves to heat skin, significantly improved hand function and decreased pain
Dietary and Lifestyle Considerations
- General aerobic exercise such as walking, swimming, and bicycling may be useful for reducing CTS symptoms.
- Better workplace ergonomics may help reduce some of the mechanical factors that precipitate job-related CTS.
Integrative Interventions
- B vitamins: CTS patients may be deficient in vitamin B6 and B12, and studies have found improvement in CTS symptoms, including less pain and better nerve conduction, with vitamin B6 and B12 supplementation.
- Alpha-lipoic acid combinations: Clinical trials using alpha-lipoic acid combined with other therapies (including curcumin and gamma-linolenic acid) have significantly improved CTS symptoms and function scores.
- Acetyl-L-carnitine: In an uncontrolled study, 1097 subjects with peripheral nerve dysfunction, including 109 subjects with CTS, were treated with intramuscular acetyl-L-carnitine daily for 10 days followed by oral acetyl-L-carnitine daily for an additional 20 days. Symptoms were rated as improved by 83% of investigators and 84% of subjects.
- Serratiopeptidase: Serratiopeptidase was given twice daily for six weeks in a clinical trial and was associated with significant clinical improvement in 65% of CTS subjects. Significant improvement in median nerve conduction velocity was also noted.
- Omega-3 fatty acids: Omega-3 fatty acids may be useful in treating CTS as molecules derived from them may block pain receptors involved in neuropathic pain.
2 Introduction
Carpal tunnel syndrome (CTS) is a relatively common disorder characterized by pain, tingling, numbness, or changes in sensation in the hands, wrists, or fingers. CTS results from irritation or compression of the median nerve, which travels from the wrist into the hand through a canal called the carpal tunnel (Marshall 2007). A significant portion of the population will be affected by CTS at some point in time, with estimates of lifetime prevalence ranging from 3-20% (LeBlanc 2011; Pajardi 2014; Haase 2007; Atroshi 1999; Ashworth 2013a; Raman 2012; Ghasemi-Rad 2014; Pandey 2013).
A variety of factors have been associated with the onset of CTS, including trauma, pregnancy, oral contraceptives, diabetes, hypothyroidism, rheumatoid arthritis, and occupational factors such as repetitive motion or use of vibrating tools. Some cases are considered idiopathic, meaning their cause is unknown (Pajardi 2014; Lewanska 2013; Alfonso 2010; Giersiepen 2011; Thomsen 2008; Eleftheriou 2012; Andersen 2011; Balci 2007; Ferry 2000). CTS is reported to be three times more common in females than males, with a reported prevalence of 3.7% among the US adult population (Ashworth 2013b).
Several treatment options are available for CTS. Corticosteroids, typically injected into the carpal tunnel, are often used in the conservative treatment of CTS; however, they may simply mask the symptoms and allow continued deterioration of the median nerve (Huisstede, Hoogvleit 2010; Marshall 2007; O’Connor 2003; Wallace 2000). Surgical release of the transverse carpal ligament is a common method of relieving moderate to severe CTS, with over 500 000 procedures performed annually in the United States (Jain 2014; A.D.A.M. 2013).
Physical medicine approaches include splints, stretching exercises, massage, ultrasound, acupuncture, and low-level laser therapy (Huisstede, Hoogvliet 2010; Huisstede, Randsdrop 2010; Fusakul 2014; Branco 1999; Baker 2012; Khosrawi 2012; Elliot 2013). Several integrative interventions such as B vitamins (especially B6), alpha-lipoic acid, omega-3 fatty acids, curcumin, and the enzyme serratiopeptidase may also be helpful in easing symptoms (Di Geronimo 2009; Pajardi 2014, Ko 2010; Ellis 1982; Panagariya 1999).
In this protocol you will learn about the causes of CTS and how this condition is conventionally diagnosed and treated. You will also discover some emerging therapies such as sonographically guided percutaneous needle release that may be effective in the management of CTS symptoms. A number of natural approaches that target some of the pathological mechanisms underlying CTS will be reviewed as well.
3 Background
The carpal tunnel is a tight passageway comprised of bone and connective tissue through which tendons and the median nerve pass. The carpal tunnel connects the forearm and the hand. Pressure within the carpal tunnel is normally between 2.5 and 15 mm Hg. Changes in nerve function begin at about 30 mm Hg, and nerve conduction is blocked when pressure exceeds 50 mm Hg. High pressure in the carpal tunnel region can cause reduced oxygen supply (hypoxia) to the median nerve and related structures. Mechanical and hypoxic stress can cause a number of harmful changes to the nerve that can lead to pain and numbness (Haase 2007; Khosrawi 2012). Many cases of CTS are related to occupations that involve forceful, repetitive use of the upper extremities. This is part of a spectrum of conditions called hand-arm vibration syndrome, in which nerves in the affected limb lose some of their protective sheath, a process known as demyelination. These structurally disturbed nerves no longer function normally (Dahlin 2014; Giersiepen 2011; Aroori 2008).
Several lines of evidence suggest that inflammation likely plays a role in the pathophysiology of CTS. For example, in one study, tenosynovial fluid samples from individuals with CTS were found to contain greater concentrations of inflammatory cells and elevated markers of oxidative stress compared to samples from people without CTS (Kim, Koh 2010; Buckley 2011). Other research shows the inflammatory enzyme cyclooxygenase-2 (COX-2), and one of its products, prostaglandin E2, may be higher in wrist tissue of CTS patients compared with those without CTS (Talmor 2003; Tucci 1997; Bland 2005a; Hirata 2004). Elevated levels of the inflammatory cytokine interleukin-6 (IL-6) have also been observed in tissue samples taken from individuals with CTS (Freeland 2002; Tucci 1997).
Cardiovascular Risk, Atherosclerosis, and Carpal Tunnel Syndrome – A Possible Connection?A cross-sectional, observational study compared 40 patients with CTS to 40 healthy controls. The researchers rigorously excluded patients with other known health problems, including cardiovascular disease, in order to avoid confounding factors. A specialized test (carotid–femoral pulse wave velocity) that measures arterial stiffness was performed on patients and controls. Carotid intima-media thickness (CIMT), another sensitive indicator of cardiovascular risk, was also measured in both groups. Arterial stiffness and CIMT were significantly greater in CTS patients compared to controls, indicating that those with CTS had greater cardiovascular risk. In fact, CIMT was an independent predictor of CTS: each 0.1 mm increase in thickness of the lining of the carotid artery doubled the likelihood of having CTS (Durakoglugil 2013). In another study, the CIMT of 58 females with CTS and no history of cardiovascular disease or stroke was compared to the CIMT of 53 healthy female controls. Maximum CIMT was significantly greater in CTS patients, and CTS was a stronger predictor of greater CIMT than age, high blood pressure, or systolic blood pressure (Park 2013). An analysis of data collected during a Finnish national health survey provided additional correlational evidence for a link between cardiovascular health and CTS. This study examined cardiovascular risk factors in relation to CTS in 6254 subjects. A number of compelling associations were revealed, with obvious age-dependency. For those aged 30-44, obesity, elevated LDL cholesterol, high triglycerides, and high blood pressure all increased the risk of CTS 2-4 times; having a cardiac arrhythmia increased the risk of CTS over 10 times. Among subjects 60 or older, heart valve disease and coronary artery disease increased CTS risk by 2.3 and 1.9 times, respectively. Moreover, for subjects 60 or older, each 0.23 mm increase in carotid intima media thickness was associated with a 40% increased chance of having CTS, but this might have been due to chance. The researchers concluded that “CTS may either be a manifestation of atherosclerosis, or both conditions may share similar risk factors” (Shiri 2011). For a detailed discussion about heart and vascular health, refer to the Atherosclerosis and Cardiovascular Disease protocol. |
4 Risk Factors
Repetitive Use and Trauma
CTS is more common in persons whose wrists and hands are exposed to repeated mechanical stress or repetitive trauma. Many studies have reported that occupational exposure to activities such as use of chainsaws or jackhammers, quarry drilling, or assembly line work increases the risk of CTS by 2- to 21-fold (Palmer 2011; Walter 2002). A study of 347 workers in a hospital and two manufacturing plants reported that working with forceful hand exertion 20-60% of the time was associated with about a 3-fold greater risk of CTS (Burt 2013).
Studies examining possible links between prolonged use of a computer keyboard or mouse and CTS have failed to consistently demonstrate significant correlation between the two. A 2014 analysis of six published CTS studies reported that computer use was non-significantly associated with higher rates of CTS (Mediouni 2014). One large study of 5658 Danish technical workers reported that while long hours of computer keyboard use was not associated with higher incidence of CTS, using a right-handed computer mouse 20 hours or more per week was associated with a significantly higher risk of right-handed CTS (Andersen 2003). Also, another researcher found that high cumulative computer keyboard strokes may increase CTS risk (Eleftheriou 2012).
CTS may also occur among musicians using repetitive hand movements, especially those who play keyboard instruments such as the piano, organ, or accordion (Wilson 2014; Lederman 2006).
Obesity
At least 18 published studies have reported an association between higher body mass index (BMI) and CTS risk (Bland 2005b). A comprehensive review of the published literature on CTS found that being overweight or obese was associated with a 40% increased chance of developing CTS (Spahn 2012). A study of the correlation between work-related hand effort and CTS found that among those with a BMI ≥ 30 (the cutoff point for obesity), there was over 3 times the odds that increased exertion would be associated with CTS (Burt 2011). This same research team later found that obese healthcare and factory workers were more than 3 times as likely to develop CTS over a 2-year follow-up period (Burt 2013). In another study, obesity increased the risk of severe CTS of unknown origin by 60%. In this study, each point increase in BMI was associated with a 9% higher risk of severe CTS; however, this elevated risk was not apparent in people over age 60 (Seror 2013). Similarly, another study reported that higher BMI was significantly associated with higher risk of CTS in 3005 adults younger than 63 years; little relationship between higher BMI and CTS was seen however in 1150 subjects over age 63 (Bland 2005b).
The mechanisms by which obesity contributes to CTS are not completely understood (Bland 2005a; Bland 2005b), and interestingly, an intervention study found that weight loss alone did not improve CTS (Kurt 2008).
Diabetes and Metabolic Syndrome
Between 11% and 25% of diabetics have CTS (Papanas 2010; Fitzgibbons 2008; Redmond 2009). CTS may occur with greater frequency in diabetics because of a number of factors, including damage to nerves resulting from high blood sugar, greater stiffness of connective tissue, and blood vessel inflammation (Dyck 1996; Ibrahim 2012; Sugimoto 2008).
A prospective survey of 676 patients found that type II diabetes increased the risk of severe CTS by 72% (Seror 2013). A study of over 100 patients with confirmed CTS found that 75% had metabolic syndrome, a condition highly correlated with future development of diabetes and cardiovascular disease. This is roughly three times the rate that would be expected in the general population. CTS patients with metabolic syndrome had more severe CTS as judged by electrophysiological parameters compared to those without CTS (Balci 2007; Beltran-Sanchez 2013). Similar results were observed in a Turkish study (Onder 2013). A population study that examined the health records of over one million people found that several factors associated with diabetes and metabolic syndrome, including gout, hypertension, and obesity, were correlated with CTS (Tseng 2012). In a case control study, CTS patients were found to have a significantly higher rate of glucose metabolism abnormalities compared to controls. The authors concluded that pre-diabetes may be a significant factor in CTS, including idiopathic CTS (Plastino 2011).
Readers may also consult the Diabetes protocol for more information.
Rheumatoid Arthritis
A strong association between CTS and rheumatoid arthritis (RA) has been observed for decades (Stevens 1992; Chamberlain 1970; Barnes 1967). The incidence of CTS in people with RA is estimated to be about 10-20% (Barnes 1967; Ashworth 2013b). CTS in RA is believed to be a result of carpal tunnel narrowing that occurs due to thickening of structures in the wrist joint (Karadag 2012; Mayo Clinic 2014).
Readers may consult the Rheumatoid Arthritis protocol for information about the disease and its treatment.
Menopause, Pregnancy, and Female Hormones
CTS is more common in women than men, and there is an apparent correlation with female sex hormones, although the exact nature of the relationship remains unclear (Kim, Hann 2010; Ferry 2000). The age of peak incidence of CTS in women is 40-60 years, which coincides with menopause (Mattioli 2008; Ashworth 2013b). An early observational study found that 17 of 53 (32%) women whose ovaries had been removed (oophorectomy) had CTS. In contrast, only 10% of premenopausal women in this study had CTS. Nerve conduction studies were abnormal in 14 of the oophorectomized women with CTS but normal in all but one of the premenopausal women. Also, symptoms were of greater severity in the oophorectomized women (Pascual 1991). Another study concluded that earlier age at menopause may increase CTS risk (Kaplan 2008). A small, uncontrolled study found that hormone replacement therapy (HRT) was effective for relieving CTS symptoms, though no nerve conduction tests were reported, and the author acknowledged the possibility of a placebo effect with HRT (Hall 1992).
CTS risk is also heightened during pregnancy, although pregnancy-related CTS is typically mild (Mondelli 2007). During pregnancy, the incidence of clinical CTS has been reported to be as high as 62% (Padua 2010). The exact cause of pregnancy-related CTS is not completely understood, but it may be related to hormonal fluctuations and accompanying fluid retention, increased weight, and/or changes in blood sugar metabolism (Osterman 2012). One study that measured improvement in CTS symptoms as well as wrist and hand functionality from pregnancy to one-year postpartum found that 40% of women experienced improvement in both measures a year after delivery (Mondelli 2007).
A large epidemiologic study compared the records of 1264 women with CTS to an equal number of women without CTS and observed that women over age 40 who had taken oral contraceptives were 38% more likely to develop CTS (Ferry 2000).
For a detailed discussion of women’s hormonal health, refer to the Female Hormone Restoration protocol.
Aromatase Inhibitors
Aromatase inhibitors (eg, anastrozole [Arimidex]), used to treat estrogen receptor-positive breast cancer (Nishihori 2008), have been associated with an increased risk of CTS. A study of over 6000 postmenopausal women who took either anastrozole or tamoxifen (Nolvadex, a selective estrogen receptor modulator) during breast cancer treatment found a highly significant difference in the rate of CTS between the two groups over a median follow-up period of over eight years. Although CTS was rare in both groups, it occurred in 2.6% of the women treated with anastrozole and 0.7% of those treated with tamoxifen. This study found that CTS rates were significantly higher in those who had previously taken HRT as well as those who had prior chemotherapy (Sestak 2009). Additionally, a case report described the onset of CTS in six women after initiation of aromatase inhibitor treatment, which was relieved when their medication was switched to tamoxifen (Nishihori 2008).
Anti-estrogen therapy, also called hormonal therapy, is used to prevent breast cancer recurrence following successful treatment; tamoxifen is often used in this setting. In a study of 4657 women who underwent successful breast cancer treatment and remained disease-free after taking tamoxifen for 2-3 years, subjects either continued taking tamoxifen or changed their treatment to the aromatase inhibitor exemestane (Aromasin). After a median 7.5-year follow-up period, women taking exemestane had over five times the chance of developing CTS during treatment than those taking tamoxifen (Mieog 2012).
Hypothyroidism
CTS appears to occur frequently in individuals with hypothyroidism (low thyroid hormone levels) (Kececi 2006). A study of over one million patient records found that hypothyroidism was correlated with CTS, and more so in individuals under the age of 39 compared to older people (Tseng 2012). The reasons for these higher rates in people with hypothyroidism are not well understood. Some research suggests that hypothyroidism may increase CTS risk by interfering with proper nerve function (Kececi 2006). However, it is not clear whether treating hypothyroidism will improve CTS symptoms; one study reported that the majority of patients treated with thyroid hormone replacement sufficient to return their thyroid hormone levels to normal continued to experience CTS symptoms (Palumbo 2000).
Other Potential Risk Factors
Trauma or burn injuries to the forearm or wrist are also potential causes of CTS (LeBlanc 2011; Hassan 2008). Leukemia, tumors, amyloidosis, sarcoidosis, or certain infections may also cause CTS (LeBlanc 2011; Hassanpour 2006; Von Glehn 2012).
CTS is relatively rare among children, but is seen in some genetic syndromes (Van Meir 2003; White 2010; Kwon 2011). Other causes of childhood CTS include wrist trauma and bone malformation (Van Meir 2003; Leduc 2014; Potulska-Chromik 2014; Davis 2014).
5 Symptoms and Diagnosis
The primary symptoms of CTS are pain, numbness, and tingling in the wrist and first three fingers of the affected hand (LeBlanc 2011; Haase 2007). Pain can also occur in the palm of the hand or in the forearm (LeBlanc 2011). Hand or wrist weakness may also be present. Symptoms involving the hands are often worse during work or at night (Haase 2007). Severe cases of CTS may be associated with visible loss of muscle mass in the hands and/or loss of ability to distinguish touch between two nearby areas of the hand (two-point discrimination) (LeBlanc 2011; Haase 2007; Kilot 2013).
Diagnostic physical exam tests include Tinel’s sign (a tingling sensation elicited by tapping over the carpal tunnel) and/or a positive Phalen’s maneuver (reproduction of symptoms, usually numbness and tingling, when the wrist is flexed) (LeBlanc 2011; Haase 2007; Szabo 1999). The “flick” signal can be a telltale sign of CTS as well; if symptomatic relief can be attained by shaking or flicking the wrist in a manner similar to shaking a thermometer, then CTS may be the cause of the symptoms (Simon 2012).
CTS can be clinically diagnosed on the basis of medical history and physical examination (LeBlanc 2011; Haase 2007; Kilot 2013), but objective testing measures such as nerve conduction studies, electromyography, and diagnostic ultrasound are commonly used as well. Nerve conduction tests are meant to detect delayed median nerve conduction rates, a diagnostic sign for CTS (LeBlanc 2011; Haase 2007). Ultrasound of the wrist joint, carpal tunnel, and median nerve can be used for CTS diagnosis (Bickel 2010; Hammer 2006; Hammer 2007), and one author suggested that ultrasound is as accurate but less expensive than nerve conduction studies (McDonagh 2014). Imaging techniques such as MRI (magnetic resonance imaging) or MRI-DTI (MRI-diffusion tensor imaging), CT (computed tomography), or X-rays may be diagnostically useful in cases involving wrist trauma, congenital abnormalities, or masses (eg, tumors) (Alfonso 2010; Haase 2007; Yildirim 2014).
6 Conventional Treatment
Conventional treatment of CTS can be conservative (eg, medication, physical therapy, corticosteroid injections) or surgical. Generally, conservative treatment is preferred for patients with mild symptoms, while surgery is considered for patients with moderate to severe pain and disability (Ghasemi-Rad 2014). A systematic review of the literature found surgical treatment yielded better results at six and 12 months than conservative medical treatment. However, the authors concluded that given evidence for the success of conservative treatment and the risk of side effects and complications from surgery, surgery should be reserved for severe and refractory cases (ie, those that do not respond to other therapies) (Shi 2011).
Medical Treatment
Corticosteroids. Corticosteroids, typically injected but sometimes taken orally, may be used to treat CTS (Ashworth 2010; Chang 1998; Marshall 2007). Injectable corticosteroids, delivered into the carpal tunnel, appear to be somewhat more effective than oral corticosteroids for alleviation of CTS symptoms, especially in the shorter term (Wong 2001; Ashworth 2010; Marshall 2007). Patients with mild CTS on the basis of nerve conduction studies appear to attain a greater duration of benefit from corticosteroid injection compared to those with moderate or severe CTS (Visser 2012). However, a potential concern with injectable corticosteroid treatment is that it may mask continued median nerve damage (Ashworth 2010). As a surgeon commented in the British Medical Journal, “Local steroid injections do not reduce the pressure on the nerve in the long term; all they do is reduce inflammation temporarily—nerve compression almost always returns” (Wallace 2000).
Non-steroidal anti-inflammatory drugs. As inflammation contributes to CTS (Ozturk 2010), oral non-steroidal anti-inflammatory drugs (NSAIDs) are sometimes used as a conservative treatment, although evidence for their effectiveness is mixed. One study compared local steroid injection to NSAID treatment in 32 CTS patients using wrist splints. Subjects who received NSAIDs exhibited improvement in some nerve conduction parameters and in their capacity to perform some intricate hand movements, such as writing and ‘stacking checkers.’ The study authors concluded that NSAIDs may be an effective treatment option when combined with wrist splinting (Gurcay 2009). A placebo-controlled trial in 73 CTS patients compared a diuretic, 20 mg/day of the NSAID tenoxicam-SR (Mobiflex), and a corticosteroid; the investigators found no significant reduction in symptoms in the diuretic or NSAID group compared to placebo (Chang 1998).
Topical treatment options. A patch containing the painkiller lidocaine (Lidoderm) was studied for the treatment of CTS-related pain. In a randomized study, adults were treated with either 5% lidocaine patches (52 subjects) or oral doses of 500 mg of naproxen (Aleve) twice daily (48 subjects). After 6 weeks of treatment, significant reductions in pain were reported in both the lidocaine- and naproxen-treated groups, with no significant difference between the two groups (Nalamachu 2006). Another study reported that treatment with EMLA cream (containing lidocaine 2.5% plus prilocaine 2.5%) for four weeks resulted in a significant reduction in pain in 30 subjects with CTS (Moghtaderi 2009).
Surgery
Surgery to relieve carpal tunnel pressure (called “carpal tunnel release”) is often used when conservative treatment fails and in severe cases. Surgery can be performed either through a standard open incision or using minimally invasive endoscopic instruments inserted through smaller incisions. Endoscopic surgery requires a 2 cm incision, shorter than traditional open CTS surgery.
Early studies comparing the two methods reported that both surgical techniques were similarly effective (Huisstede, Randsdrop 2010), though some more recent research has indicated that new endoscopic CTS surgery techniques may produce better results than traditional open CTS surgery. In one study, CTS symptoms six and 12 months after surgery were significantly improved in 60 subjects who underwent endoscopic surgery compared to 60 subjects who received standard open CTS surgery. The average time to return to work was 16.6 days in the endoscopic group compared to 25.4 days in the standard surgical group. In addition, scar healing was judged by patients to be significantly better in the endoscopic group compared to standard open surgery (Tarallo 2014). Attempts to develop sonographically-guided endoscopic surgical methods to further decrease trauma from surgery, by using a surgical incision of just 1 mm, have been reported (Rojo-Manaute 2013; de la Fuente 2013).
A rigorous review and analysis of the scientific literature compared endoscopic surgery to any other surgical treatment of CTS. The authors found no difference in relief of symptoms, return to functional status, or rate of major complications between the methodologies. Endoscopy, however, showed some superiority in terms of incidence of minor complications and improvement in grip strength, and resulted in a quicker return to work (Vasiliadis 2014).
Physical and Mechanical Treatment Modalities
A variety of physical and mechanical measures have demonstrated benefit for relief and rehabilitation from CTS, including splints and immobilization, home exercises (eg, stretching), massage, and certain types of manipulative and mobilization therapies (Kilot 2013; Kostopoulos 2004).
Splinting. Use of splints that hold the wrist in a neutral position are often recommended for CTS, but evidence in support of this approach is of low quality (Baker 2012; LeBlanc 2011; Page 2012). Splinting may be combined with other treatment modalities, such as stretching and acupuncture. One study of 40 patients recovering from CTS surgery found that splinting was of no benefit, and bulky dressings may be more comfortable, as effective, and less expensive for post-surgical recovery in CTS compared to splinting (Cebesoy 2007).
A study compared four weeks of splinting devices and stretching exercises in 124 adults with mild-to-moderate CTS. Researchers compared a conventional splint to a “lumbrical splint” and standard general hand and wrist stretching exercises to another set of stretching exercises designed to reduce tightness of the lumbrical muscles (muscles of the hand). Subjects received standard or lumbrical splints and instructions to perform either standard or lumbrical stretching exercises. After treatment, CTS symptoms improved significantly with all treatments; however, the best results were seen in subjects receiving standard splints combined with lumbrical stretching (Baker 2012).
Massage. Massage therapy has been the subject of several CTS trials. One trial that tested six weeks of twice-weekly massage and trigger-point therapy in 21 people with CTS reported significant improvement in symptom severity as well as functional ability of the hand and wrist (Elliot 2013). An earlier study compared six weeks of twice-weekly 30-minute sessions of general massage to carpal-tunnel-targeted massage. Targeted massage therapy resulted in a significant 17.3% increase in grip strength compared to a 4.8% increase in the general massage group (Moraska 2008). A randomized, controlled trial compared splinting plus self-massage to splinting alone. Both groups had six months of splinting, with the self-massage group self-treating for six weeks. Both grip strength and patient-physician assessment of CTS symptoms improved to a significantly greater extent in the subjects who underwent splinting and self-massage compared to those utilizing splinting alone (Madenci 2012).
Manipulation and mobilization techniques. When performed by a skilled practitioner, manual manipulation of the structures of and surrounding the carpal tunnel, including bones, tendons, ligaments, and muscles, may relieve CTS symptoms. Such treatments are meant to increase the volume of the carpal tunnel by increasing the length of the transverse carpal ligament, thus decreasing pressure on the median nerve (Schreiber 2014; Sucher 1998; Sucher 2012; Siu 2012). Some physical medicine practitioners report that mobilization of the involved nerve itself has produced symptomatic improvement (Kostopoulos 2004).
Transcutaneous Electrical Nerve Stimulation
Transcutaneous electrical nerve stimulation (TENS) involves passing low-intensity electrical current through the skin to stimulate nerves. It has been studied, with reported success, in a variety of medical pain management settings; however, further high quality controlled studies are necessary to conclusively demonstrate its efficacy (Sbruzzi 2012; Proctor 2002; Bennett 2011; Robb 2008; Osiri 2000). TENS treatment may reduce inflammation and stimulate ATP production (Branco 1999; Naeser 2002). (ATP is a critical cellular energy reservoir used throughout the body.) In a double-blind, placebo-controlled study, 11 subjects with borderline-mild or moderate CTS were treated with red-beam laser therapy, infrared laser therapy, and TENS or sham/placebo treatment three times weekly for 3-4 weeks in random sequence. After active treatment, signs and symptoms of CTS were significantly reduced compared to sham treatment (Naeser 2002). Another study on 31 subjects with CTS, some of whom had involvement of both hands, reported that 4-5 weeks of combined red-beam laser and TENS treatment resulted in significant reduction in wrist pain (Branco 1999).
7 Novel and Emerging Strategies
Sonographically Guided Percutaneous Needle Release
Carpal tunnel release surgery, whether traditional or endoscopic (minimally invasive), poses greater risk than conservative treatment. Sonographically guided percutaneous needle release is an innovative method that uses ultrasound to visualize the wrist while a fine needle decompresses the carpal tunnel by releasing the transverse carpal ligament. This approach may provide similar results to minimally invasive surgery with lower risk and recovery time (Schreiber 2014; McShane 2012; Kerasnoudis 2012; Nakamichi 2010). Additional controlled studies are needed to confirm the potential of this treatment.
Low-Level Laser Therapy
An interesting approach to treating CTS involves the use of a low-level (low-power) laser, known as low-level laser therapy (LLLT), to stimulate the median nerve (Fusakul 2014). This modality has shown an ability to enhance some aspects of median nerve function (Basford 1993). Several clinical studies have shown LLLT improves various symptoms related to CTS. One study showed LLLT to be as effective as surgical treatment for mild-to-moderate CTS, while another demonstrated the procedure to be as cost-effective as surgery (Elwakil 2007; Chang 2008; Evcik 2007; Shooshtari 2008; Fusakul 2014). Observed benefits of LLLT include:
- Improved grip strength (Evcik 2007; Shooshtari 2008; Fusakul 2014)
- Alleviation of pain (Chang 2008; Dakowicz 2011)
- Improved nerve conduction study parameters (Yagci 2009; Shooshtari 2008; Fusakul 2014)
- Reduction of paresthesia (tingling) and numbness (Shooshtari 2008)
Microwave Heat Treatment
Microwave hypothermia, which uses microwaves to heat the skin to about 39.7°C (103.5°F), may be helpful for CTS. A 2011 trial used microwave hyperthermia to treat 22 subjects with mild-to-moderate CTS. Over three weeks, 11 subjects underwent six microwave hyperthermia treatments and 11 underwent six sham (placebo) treatments. After three weeks, significant reductions in pain and significant improvements in hand function were reported in the microwave hyperthermia-treated group but not in the sham-treated group (Frasca 2011).8 Lifestyle Considerations
Exercise
General aerobic exercise such as walking, swimming, and bicycling may be useful for reducing CTS symptoms. A study of 30 adults with CTS found that participation in a supervised aerobic exercise program for 10 months reduced pain, tightness, and improved fine motor skills (Nathan 2001). In one preliminary trial, yoga was found to relieve some CTS signs and symptoms more effectively than splinting (Garfinkel 1998).
Improved Ergonomics
Better workplace ergonomics may help reduce or relieve some of the mechanical factors that precipitate occupationally-induced CTS. In jobs involving excessive wrist bending and hand-arm vibration, efforts to reduce CTS risk include proper posture; proper training to ensure that optimal workplace ergonomics are applied; an introduction period during which new employees can acclimate to job tasks; proper tool size and power relative to the worker using the equipment; regular breaks and changes in types of hand movements to reduce repetitive trauma; ergonomically optimized tool design that reduces force exerted on the wrist; and tool vibration dampening techniques (Palmer 2011).
Despite a number of studies that have attempted to identify a causative role of excessive computer usage in CTS, computer keyboard use has not been confirmed as an etiologic factor. Nevertheless, some researchers advise that when using computer keyboards, hands should be placed in a “neutral position” in which the wrist is extended (bent backward) no more than 20o (Rempel 2008; Keir 2007).
9 Nutrients
Vitamin B6
Reported Dosage: 50–200 mg/day (as pyridoxine)
Vitamin B6 plays an essential role in amino acid metabolism, neurotransmitter synthesis, and nerve function. Vitamin B6 deficiency has long been suspected as a contributing factor in some cases of carpal tunnel syndrome (Fuhr 1989; Gaby 2023), although not all trials have demonstrated consistent benefit.
Evidence from several studies suggests vitamin B6 supplementation may improve CTS symptoms (Gaby 2023; Talebi 2013; Bernstein 1993; Ellis 1982). In a randomized controlled trial including 40 patients with mild-to-moderate CTS, participants received wrist splinting with or without vitamin B6 supplementation (120 mg daily) for three months. Patients receiving vitamin B6 experienced significant reduction in symptoms of pain, numbness, weakness, and nocturnal awakening, compared with splinting alone. Sensory nerve conduction velocity also improved significantly in the vitamin B6 group (Talebi 2013). Sensory nerve conduction velocity measures how quickly electrical signals travel along the sensory fibers of the median nerve, and slowing of this conduction is a common physiological finding in carpal tunnel syndrome.
Evidence on the use of vitamin B6 in the management of carpal tunnel syndrome dates back several decades. Early observational studies, uncontrolled trials, and small double-blind crossover studies reported that some individuals with CTS had low vitamin B6 status and experienced improvements in symptoms, pain, and nerve conduction with supplementation in the range of approximately 50–200 mg/day. These findings were reported particularly in patients with documented vitamin B6 deficiency and helped generate early interest in the potential role of pyridoxine in CTS management (Gaby 2023; Bernstein 1993; Ellis 1982; Ellis 1981; Keniston 1981).
Note: The research on CTS mentioned here (and below in the “Other B Vitamins” section) used vitamin B6 in the form of pyridoxine. However, high-dose pyridoxine has been linked to sensory neuropathy in some studies. For this reason, Life Extension generally prefers the pyridoxal-5’-phosphate form of B6 (Hemminger 2026).
Other B Vitamins
Reported Dosage: Riboflavin (Vitamin B2): 50 mg/day
Vitamin B6 metabolism also depends on adequate status of other B vitamins, particularly riboflavin (vitamin B2), which is required for the conversion of vitamin B6 to its active coenzyme form, pyridoxal-5’-phosphate (Jungert 2020). Insufficient riboflavin status may therefore impair vitamin B6 utilization even when vitamin B6 intake is adequate. Supporting overall B-vitamin status may therefore be important when considering nutritional strategies aimed at improving nerve function and metabolic processes involved in CTS.
In a 1984 case report of a patient with CTS who showed functional deficiencies of riboflavin and vitamin B6, supplementation with 50 mg/day riboflavin for five months led to near resolution of symptoms. Next, researchers gave the patient riboflavin (50 mg/day) and pyridoxine therapy (500 mg/day) for three months, which led to complete symptom resolution and improved grip strength. Surgery was no longer needed (Folkers 1984).
Combination formulas containing B vitamins have shown benefits for CTS (see “Nutrient Combinations” section).
Lipoic Acid
Reported Dosage: R-lipoic acid, 600 mg/day
Alpha-lipoic acid is an antioxidant and anti-inflammatory compound that has been widely studied in the context of peripheral neuropathy. Randomized trials and meta-analyses have demonstrated improvements in neuropathic symptoms and nerve function in people with diabetic and other peripheral neuropathies (Memeo 2008; Mijnhout 2010; Reljanovic 1999; Ziegler 2006; Ziegler 2004). Lipoic acid has also been shown in both a preclinical cell study and clinical trial to reduce inflammatory signaling and cytokines such as IL-6 (Salinthone 2010; Zhang 2011), which could contribute to nerve irritation, swelling, and pain.
Lipoic acid has shown promise in individuals with CTS. In a prospective, open-label, randomized study of 134 patients with mild-to-moderate CTS, participants received either supplementation with 600 mg/day of R-lipoic acid for 60 days or no intervention. (The “R” form of lipoic acid is the naturally occurring form, whereas alpha-lipoic acid contains both the “R” and “S” forms; the “S” form is not naturally occurring.) (Teichert 2003; Uchida 2015). Patients receiving R- lipoic acid experienced significantly greater reductions in pain compared with controls, although no significant improvements in other Boston Carpal Tunnel Questionnaire symptom or functional scores were found (Passiatore 2020).
In a 90-day open-label comparative study, 112 adults with moderately severe carpal tunnel syndrome received either an oral combination providing 600 mg alpha-lipoic acid plus 360 mg gamma-linolenic acid daily, along with selenium, vitamin E, and several B vitamins, or a B-complex preparation. Compared with the B-complex group, the alpha-lipoic acid/gamma-linolenic acid group had larger improvements on the Boston Carpal Tunnel Questionnaire—the study’s main symptom and function measure—and showed improvement on the historical-objective (Hi-Ob) clinical scale and an electrophysiology-based CTS severity scale after 90 days. The percentage of patients considered surgical candidates also fell from about 77% to 50% in the combination group versus 82% to 70% in the B-complex group. However, this result is hard to interpret because the study was unblinded, used a multi-ingredient product, and did not clearly report randomization or other key methods that reduce bias. Overall, this study suggests possible short-term benefits of this specific combination in carpal tunnel syndrome, but its design limitations mean it does not provide strong evidence that alpha-lipoic acid alone is effective (Di Geronimo 2009).
Vitamin D
Reported Dosage: 50–150 mcg/day (2,000–6,000 IU/day) OR 1,250–1,500 mcg/week (50,000–60,000 IU/week)
Vitamin D plays a role in immune modulation, inflammation control, and nerve health (Shi 2024). Emerging evidence suggests vitamin D deficiency may worsen neuropathic pain and contribute to carpal tunnel syndrome symptoms, as patients with CTS and low vitamin D levels have been reported to experience greater pain and symptom severity, with improvements observed following vitamin D supplementation (Andrade 2024; Samant 2022). “Low levels” of vitamin D include deficiency (serum 25-hydroxyvitamin D [25(OH)D] levels <20 ng/mL) as well as insufficiency (serum levels of 20–29 ng/mL), as defined by the Endocrine Society (Holick 2011).
Vitamin D supplementation has been shown to improve pain and nerve function in patients with carpal tunnel syndrome and vitamin D deficiency. In a randomized clinical study, 14 women with CTS and vitamin D insufficiency (about 26 ng/mL in the control group and 23 ng/mL in the treatment group) received either corticosteroid treatment alone (control group) or corticosteroid therapy combined with 50 mcg (2,000 IU) vitamin D (form not specified) supplementation daily. Patients receiving the corticosteroid with vitamin D experienced significant reductions in pain, whereas the control group did not experience a significant reduction. Both groups experienced reductions in symptom severity, though not functional improvement (Andrade 2024).
In an uncontrolled open-label study of 50 women with mild-to-moderate carpal tunnel syndrome and vitamin D deficiency, replenishing vitamin D with 150 mcg (6,000 IU)/day or 1,250 mcg (50,000 IU)/week of vitamin D2 or D3 significantly improved pain scores and electrophysiological measures of nerve function, although multiple dosing regimens were used and outcomes were not analyzed separately by dose or form, which limits conclusions about optimal dosing (Saçmaci 2020).
Similar findings were reported in a prospective pre-post clinical study without a control group of 42 patients with CTS, in which vitamin D3 supplementation (1,500 mcg [60,000 IU/weekly]) for three months significantly reduced pain and improved Boston Carpal Tunnel Questionnaire symptom and functional scores (Samant 2022).
Overall, current evidence for vitamin D supplementation in CTS comes from trials in patients with documented vitamin D deficiency or insufficiency; whether supplementation benefits vitamin D-replete individuals with CTS is unknown.
Acetyl-L-Carnitine
Reported Dosage: 500–1,000 mg/day
Acetyl-L-carnitine (ALC) supports mitochondrial energy metabolism and has demonstrated neuroprotective and analgesic effects in several studies of peripheral neuropathy. Preclinical and clinical research suggests ALC may promote nerve regeneration, improve mitochondrial function, and reduce neuropathic pain (Memeo 2008; Chiechio 2006; De Grandis 2002; Flatters 2006).
A multicenter clinical study that was examiner-blinded, but not randomized or controlled, investigated the effects of acetyl-L-carnitine in 82 patients with mild-to-moderate CTS. Participants received injections of 500 mg twice daily for 10 days, followed by 500 mg twice/day orally for 110 days. Treatment resulted in significant improvements in several clinical measures, including Boston Carpal Tunnel Questionnaire scores and neuropathic pain symptoms. Electrophysiological testing also demonstrated improvements in sensory nerve conduction velocity, although the study was a single-arm design with no control group which substantially limits interpretability of the findings (Cruccu 2017).
In patients with neuropathic pain associated with rheumatoid or spondyloarthritis, a controlled clinical study evaluated a branded combination of 600 mg palmitoylethanolamide and 500 mg of acetyl-L-carnitine (Kalanit) given twice daily for two weeks, then once daily for a 6-month period thereafter. Of the 31 patients in a CTS subgroup, 16 received the supplement combination along with standard therapy and reported significantly reduced pain when compared with 15 controls on standard therapy alone (Parisi 2021).
Combination formulas with acetyl-L-carnitine have been reported to be successful at improving symptoms of CTS (discussed in “Nutrient Combinations” below).
Palmitoylethanolamide (PEA)
Reported Dosage: 600–1,200 mg/day
Palmitoylethanolamide (PEA) has been investigated (individually and in combination with other nutrients) in carpal tunnel syndrome due to its anti-inflammatory and neuroprotective properties.
Evidence suggests PEA may favorably impact outcomes. In a randomized controlled trial published in 2011, 26 patients with moderate CTS received 600 or 1,200 mg PEA daily for 30 days compared with a no-treatment control group. The investigators reported significant improvements in median nerve distal latency, along with reductions in Tinel’s sign and discomfort symptoms. Notably, the 1,200 mg/day dosage produced greater improvements than the 600 mg/day dosage, suggesting a dose-dependent effect (Conigliaro 2011). A study published in 2017 found that 600 mg per day of PEA did not improve symptoms compared with placebo. Together, these studies suggest that 1,200 mg/day PEA may be more appropriate in the context of CTS (Faig-Martí 2017).
Additional data comes from a randomized, controlled, open-label trial examining 42 CTS patients awaiting surgical decompression who experienced significant pain and sleep disturbance. Participants received 600 mg ultramicronized PEA twice daily before and after surgery, while the control group underwent surgery alone. The PEA group experienced significant improvements in sleep quality and pain symptoms prior to surgery, evidence that PEA may provide symptomatic relief in patients with severe carpal tunnel syndrome awaiting surgery (Evangelista 2018).
Also, patients with CTS who received 600 mg PEA together with 500 mg acetyl-L-carnitine (Kalanit) showed significant pain reductions after six months (summarized earlier in the “Acetyl-L-Carnitine” section) (Parisi 2021).
Omega-3 Fatty Acids
Reported Dosage: 3,000 mg/day combined EPA plus DHA
Omega-3 fatty acids, particularly the long-chain fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), have anti-inflammatory and neuroprotective properties that may be relevant to inflammatory changes and mechanical compression of the median nerve seen in CTS. These fatty acids have been implicated in nerve injury and inflammation, reduction of inflammatory eicosanoids, modulation of cytokine production, and support of neuronal membrane integrity (Calder 2017). Further, EPA and DHA are precursors to specialized pro-resolving mediators (SPMs), which help resolve inflammation and promote tissue repair (Xu 2010).
Evidence from a controlled clinical trial has demonstrated that omega-3 supplementation improved symptoms in CTS. The randomized controlled trial evaluated the effects of omega-3 fatty acid administration in 28 patients with mild-to-moderate carpal tunnel syndrome. In this double-blind study, participants were assigned to receive either fish oil supplementation or placebo for three months in addition to a B complex. The fish oil groups received either 1,200 mg/day or 3,000 mg/day of a combined EPA:DHA ratio of 1:5. At the end of the study period, the 10 patients who received 3,000 mg/day experienced significantly greater reductions in pain and numbness compared with placebo, with mean pain scores decreasing by approximately 0.8 points per month. No serious adverse effects were reported during treatment (Paecharoen 2020).
Nutrient Combinations
Because carpal tunnel syndrome involves multiple biological processes including inflammation, oxidative stress, and impaired nerve metabolism, nutrient combinations have been investigated as a strategy to support several therapeutic targets simultaneously.
In a randomized open-label prospective study involving 147 patients awaiting surgery for mild-to-moderate CTS, participants received a combination supplement containing a total of 600 mg twice daily (alpha-lipoic acid, acetyl-L-carnitine, curcumin, phosphatidylserine, and multiple vitamins C, E and B-group vitamins]) (at undisclosed individual quantities) for 60 days. The intervention significantly improved Boston Carpal Tunnel Questionnaire symptom scores and reduced pain levels compared with baseline, although functional scores showed no meaningful improvement (D’Orio 2023).
Supplementation before and after surgery with alpha-lipoic acid, curcumin phytosome, and B vitamins may help improve postoperative symptom recovery in CTS patients undergoing surgery. In a randomized controlled trial, 180 CTS patients scheduled for surgical decompression were divided into three groups of 60 each: a control group receiving no supplementation, a group receiving a combination supplement both before and after surgery for a total of six months, and a group receiving the supplement for three months before surgery only. The supplement (Axin C) provided 300 mg alpha-lipoic acid, 500 mg curcumin phytosome, 1.05 mg vitamin B1, 1.2 mg vitamin B2, 4.5 mg vitamin B5, and 1.5 mg vitamin B6 per tablet, taken twice daily. Patients who received supplementation both before and after surgery had significantly lower nocturnal symptom scores at 40 days and three months after surgery, and fewer positive Phalen’s tests (measure of the pressure on the median nerve in the wrist) at three months, compared with controls (Pajardi 2014).
Disclaimer and Safety Information
This information (and any accompanying material) is not intended to replace the attention or advice of a physician or other qualified health care professional. Anyone who wishes to embark on any dietary, drug, exercise, or other lifestyle change intended to prevent or treat a specific disease or condition should first consult with and seek clearance from a physician or other qualified health care professional. Pregnant women in particular should seek the advice of a physician before using any protocol listed on this website. The protocols described on this website are for adults only, unless otherwise specified. Product labels may contain important safety information and the most recent product information provided by the product manufacturers should be carefully reviewed prior to use to verify the dose, administration, and contraindications. National, state, and local laws may vary regarding the use and application of many of the therapies discussed. The reader assumes the risk of any injuries. The authors and publishers, their affiliates and assigns are not liable for any injury and/or damage to persons arising from this protocol and expressly disclaim responsibility for any adverse effects resulting from the use of the information contained herein.
The protocols raise many issues that are subject to change as new data emerge. None of our suggested protocol regimens can guarantee health benefits. Life Extension has not performed independent verification of the data contained in the referenced materials, and expressly disclaims responsibility for any error in the literature.
A.D.A.M. New York Times Health Guide. Health page. Carpal Tunnel Syndrome. Available at: http://www.nytimes.com/health/guides/disease/carpal-tunnel-syndrome/surgery.html. 7/14/2013. Accessed 9/23/2014.
Alfonso C, Jann S, Massa R, Torreggiani A. Diagnosis, treatment and follow-up of the carpel tunnel syndrome: a review. Neurological Sci 2010;31:243-252.
Andersen JH, Fallentin N, Thomsen JF, Mikkelsen S. Risk factors for neck and upper extremity disorders among computers users and the effect of interventions: an overview of systematic reviews. PloS one. 2011;6(5):e19691.
Andersen JH, Thomsen JF, Overgaard E, Lassen CF, Brandt LPA, Vilstrup I, et al. Computer use and carpal tunnel syndrome: a 1-year follow-up study. JAMA 2003;289:2963-2969.
Andrade AVD, Martins DGS, Rocha GS, et al. The Role of Vitamin D in the Treatment of Carpal Tunnel Syndrome: Clinical and Electroneuromyographic Responses. Nutrients. Jun 19 2024;16(12)doi:10.3390/nu16121947. https://www.ncbi.nlm.nih.gov/pubmed/38931299
Aroori S, Spence RA. Carpal tunnel syndrome. The Ulster medical journal. Jan 2008;77(1):6-17.
Ashworth N. Carpal tunnel syndrome. Clinical Evidence 2010;1114.
Ashworth N. ePocrates online. Diseases page. Carpal tunnel syndrome. Available at: https://online.epocrates.com/noFrame/showPage.do?method=diseases&MonographId=380. Last updated 4/5/2013b. Accessed 4/16/2014.
Ashworth NL. Medscape online. Carpal Tunnel Syndrome. Available at: http://emedicine.medscape.com/article/327330-overview. Last updated 3/5/2013a. Accessed 4/16/2014.
Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosen I. Prevalence of carpal tunnel syndrome in a general population. JAMA: the journal of the American Medical Association. Jul 14 1999;282(2):153-158.
Baker NA, Moehling KK, Rubinstein EN, Wollstein R, Gustafson NP, Baratz M. The comparative effectiveness of combined lumbrical muscle splints and stretches on symptoms and function in carpal tunnel syndrome. Arch Phys Med Rehabil 2012;93:1-9.
Balci K, Utku U. Carpal tunnel syndrome and metabolic syndrome. Acta Neurol Scand 2007; 116:113-117.
Barnes CG, Currey HL. Carpal tunnel syndrome in rheumatoid arthritis. A clinical and electrodiagnostic survey. Annals of the rheumatic diseases. May 1967;26(3):226-233.
Basford JR, Hallman HO, Matsumoto JY, Moyer SK, Buss JM, Baxter GD. Effects of 830 nm continuous wave laser diode irradiation on median nerve function in normal subjects. Lasers in surgery and medicine. 1993;13(6):597-604.
Beltran-Sanchez H, Harhay MO, Harhay MM, McElligott S. Prevalence and trends of metabolic syndrome in the adult U.S. population, 1999-2010. Journal of the American College of Cardiology. Aug 20 2013;62(8):697-703.
Bennett MI, Hughes N, Johnson MI. Methodological quality in randomised controlled trials of transcutaneous electric nerve stimulation for pain: low fidelity may explain negative findings. Pain. Jun 2011;152(6):1226-1232.
Bernstein AL, Dinesen JS. Brief communication: effect of pharmacological doses of vitamin B6 on carpal tunnel syndrome, electroencephalographic results, and pain. J Am Coll Nutr 1993;12:73-76.
Bickel KD, Carpal tunnel syndrome. J Hand Surgery 2010;35:147-152.
Bland JDP. Carpal tunnel syndrome. Curr Opin Neurol 2005a;18:581-585.
Bland JDP. The relationship of obesity, age, and carpal tunnel syndrome: More complex than was thought? Muscle Nerve 2005b;32:527-32.
Branco K, Naeser MA. Carpal tunnel syndrome: Clinical outcome after low-level laser acupuncture, microamps transcutaneous electrical nerve stimulation, and other alternative therapies-an open protocol study. J Altern Compliment Med 1999;5:5-26.
Buckley CD. Why does chronic inflammation persist: An unexpected role for fibroblasts. Immunology letters. Jul 2011;138(1):12-14.
Burt S, Crombie K, Jin Y, Wurzelbacher S, Ramsey J, Deddens J. Workplace and individual risk factors for carpal tunnel syndrome. Occupational and environmental medicine. Dec 2011;68(12):928-933.
Burt S, Deddens JA, Crombie K, Jin Y, Wuerzelbacher S, Ramsey J. A prospective study of carpal tunnel syndrome: workplace and individual risk factors. Occup Environ Med 2013;70:568-574.
Calder PC. Omega-3 fatty acids and inflammatory processes: from molecules to man. Biochem Soc Trans. Oct 15 2017;45(5):1105-1115. doi:10.1042/bst20160474.
Cebesoy O, Kose KC, Kuru I, Altinel L, Gul R, Demirtas M. Use of a splint following open carpal tunnel release: A comparative study. Advances Therapy 2007;24:478-484.
Chamberlain MA, Corbett M. Carpal tunnel syndrome in early rheumatoid arthritis. Annals of the rheumatic diseases. Mar 1970;29(2):149-152.
Chang MH, Chiang HT, Lee SS, Ger LP, Lo YK. Oral drug of choice in carpal tunnel syndrome. Neurology 1998;51:390-393.
Chang WD, Wu JH, Jiang JA, Yeh CY, Tsai CT. Carpal tunnel syndrome treated with a diode laser: a controlled treatment of the transverse carpal ligament. Photomedicine and laser surgery. Dec 2008;26(6):551-557.
Chiechio S, Copani A, Nicoletti F, Gereau RWt. L-acetylcarnitine: a proposed therapeutic agent for painful peripheral neuropathies. Current neuropharmacology. Jul 2006;4(3):233-237.
Conigliaro R, Drago V, Foster PS, Schievano C, Di Marzo V. Use of palmitoylethanolamide in the entrapment neuropathy of the median in the wrist. Minerva Med. Apr 2011;102(2):141-7. https://www.ncbi.nlm.nih.gov/pubmed/21483401
Cruccu G, Di Stefano G, Fattapposta F, et al. L-Acetyl-carnitine in Patients with Carpal Tunnel Syndrome: Effects on Nerve Protection, Hand Function and Pain. CNS drugs. Dec 2017;31(12):1103-1111. doi:10.1007/s40263-017-0476-2. https://link.springer.com/content/pdf/10.1007/s40263-017-0476-2.pdf
Dahlin LB, Sanden H, Dahlin E, Zimmerman M, Thomsen N, Bjorkman A. Low myelinatinated nerve-fibre density may lead to symptoms associated with nerve entrapment in vibration-induced neuropathy. J Occupational Med Toxicol 2014;9:7.
Dakowicz A, Kuryliszyn-Moskal A, Kosztyla-Hojna B, Moskal D, Latosiewicz R. Comparison of the long-term effectiveness of physiotherapy programs with low-level laser therapy and pulsed magnetic field in patients with carpal tunnel syndrome. Advances in medical sciences. 2011;56(2):270-274.
Davis L, Vedanarayanan VV. Carpal tunnel syndrome in children. Pediatric neurology. Jan 2014;50(1):57-59.
De Grandis D, Minardi C. Acetyl-L-carnitine (levacecarnine) in the treatment of diabetic neuropathy. A long-term, randomised, double-blind, placebo-controlled study. Drugs in R&D. 2002;3(4):223-231.
de la Fuente J, Miguel-Perez MI, Balius R, Guerrero V, Michaud J, Bong D. Minimally invasive ultrasound-guided carpal tunnel release: a cadaver study. Journal of clinical ultrasound: JCU. Feb 2013;41(2):101-107.
Di Geronimo G, Caccese AF, Caruso L, Soldait A, Passaretti U. Treatment of carpal tunnel syndrome with alpha-lipoic acid. Eur Rev Med Pharmacol Sci 2009;13:133-139.
D'Orio M, De Vitis R, Taccardo G, et al. Clinical usefulness of nutraceutics with acetyl-L-carnitine, α-lipoic acid, phosphatidylserine, curcumin, C, E and B-group vitamins in patients awaiting for carpal tunnel release during COVID-19 pandemic: a randomized controlled open label prospective study. Acta bio-medica : Atenei Parmensis. Jun 23 2023;94(S2):e2023050. doi:10.23750/abm.v94iS2.12513. https://mattioli1885journals.com/index.php/actabiomedica/article/download/12513/10424
Durakoglugil ME, Cieck Y, Kocaman SA, Balik S, Kirbas S, Cetin M, et al. Increased pulse wave velocity and carotid intima-media thickness in patients with carpal tunnel syndrome. Muscle Nerve 2013;47:872-877.
Dyck PJ, Giannini C. Pathologic alterations in the diabetic neuropathies of humans: a review. Journal of neuropathology and experimental neurology. Dec 1996;55(12):1181-1193.
Eleftheriou A, Rachiotis G, Varitimidis S, Koutis C, Malizos KN, Hadjichristodoulou C. Cumulative keyboard strokes: a possible risk factor for carpal tunnel syndrome. Journal of occupational medicine and toxicology (London, England). 2012;7(1):16.
Elliot R, Burkett B. Massage therapy as an effective treatment for carpal tunnel syndrome. J Bodywork Movement Therap 2013;17:332-338.
Ellis JM, Folkers K, Levy M, Shizukuishi S, Lawandski J, Nishii S, et al. Response of vitamin B-6 deficiency and the carpal tunnel syndrome to pyridoxine. Proc Natl Acad Sci USA 1982;79:7494-7498.
Ellis JM, Folkers K, Levy M, Takemura K, Shizukuishi S, Ulrich R, et al. Therapy with vitamin B6 with and without surgery for treatment of patients having idiopathic carpal tunnel syndrome. Res Commun Chem Pathol Pharmacol 1981;33:331-334.
Elwakil TF, Elazzazi A, Shokeir H. Treatment of carpal tunnel syndrome by low-level laser versus open carpal tunnel release. Lasers in medical science. Nov 2007;22(4):265-270.
Evangelista M, Cilli, De Vitis R, Militerno A, Fanfani F. Ultra-micronized Palmitoylethanolamide Effects on Sleep-wake Rhythm and Neuropathic Pain Phenotypes in Patients with Carpal Tunnel Syndrome: An Open-label, Randomized Controlled Study. CNS & neurological disorders drug targets. 2018;17(4):291-298. doi:10.2174/1871527317666180420143830. https://www.ncbi.nlm.nih.gov/pubmed/29676237
Evcik D, Kavuncu V, Cakir T, Subasi V, Yaman M. Laser therapy in the treatment of carpal tunnel syndrome: a randomized controlled trial. Photomedicine and laser surgery. Feb 2007;25(1):34-39.
Faig-Martí J, Martínez-Catassús A. Use of palmitoylethanolamide in carpal tunnel syndrome: a prospective randomized study. J Orthop Traumatol. Dec 2017;18(4):451-455. doi:10.1007/s10195-017-0453-z. https://link.springer.com/content/pdf/10.1007/s10195-017-0453-z.pdf
Ferry S, Hannaford P, Warskyj M, Lewis M, Croft P. Carpal tunnel syndrome: a nested case-control study of risk factors in women. American journal of epidemiology. Mar 15 2000;151(6):566-574.
Fitzgibbons PG, Weiss APC. Hand manifestations of Diabetes Mellitus. J Hand Surg 2008;33A:771-775.
Flatters SJ, Xiao WH, Bennett GJ. Acetyl-L-carnitine prevents and reduces paclitaxel-induced painful peripheral neuropathy. Neuroscience letters. Apr 24 2006;397(3):219-223.
Folkers K, Wolaniuk A, Vadhanavikit S. Enzymology of the response of the carpal tunnel syndrome to riboflavin and to combined riboflavin and pyridoxine. Proc Natl Acam Sci USA 1984;81:7076-7078.
Frasca G, Maggi L, Padua L, Ferrara PE, Granata G, Minciotti I, et al. Short-term effects of local microwave hyperthermia on pain and function in patients with mild to moderate carpal tunnel syndrome: a double blind randomized sham-controlled trial. Clinical Rehabilitation 2011;25:1109-1118.
Freeland AE, Tucci MA, Barbieri RA, Angel MF, Nick TG. Biochemical evaluation of serum and flexor tenosynovium in carpal tunnel syndrome. Microsurgery. 2002;22(8):378-385.
Fuhr JE, Farrow A, Nelson HS, Jr. Vitamin B6 levels in patients with carpal tunnel syndrome. Archives of surgery (Chicago, Ill. : 1960). Nov 1989;124(11):1329-1330.
Fusakul Y, Aranyavalai T, Saensri P, Thiengwittayaporn S. Low-level laser therapy with a wrist splint to treat carpal tunnel syndrome: a double-blinded randomized controlled trial. Lasers Med Sci. May 2014;29(3):1279-1287.
Gaby A. Nutritional Medicine (e3). Chapter 129: Carpal Tunnel Syndrome. 2023.
Garfinkel MS, Singhal A, Katz WA, Allan DA, Reshetar R, Schumacher HR, Jr. Yoga-based intervention for carpal tunnel syndrome: a randomized trial. JAMA: the journal of the American Medical Association. Nov 11 1998;280(18):1601-1603.
Ghasemi-Rad M, Nosair E, Vegh A, Mohammadi A, Akkad A, Lesha E, . . . Hasan A. A handy review of carpal tunnel syndrome: From anatomy to diagnosis and treatment. World journal of radiology. Jun 28 2014;6(6):284-300.
Giersiepen K, Spallek M. Carpal tunnel syndrome as an occupational disease. Deutsches Arzteblatt international. Apr 2011;108(14):238-242.
Gurcay E, Unlu E, Gurcay AG, Tuncay R, Cakci A. Evaluation of the effect of local corticosteroid injection and anti-inflammatory medication in carpal tunnel syndrome. Scottish medical journal. Feb 2009;54(1):4-6.
Haase J. Carpel tunnel syndrome - a comprehensive review. Advances Technical Standards Neurosurgery 2007;32:178-249.
Hall GM, Spector TD, Studd JW. Carpal tunnel syndrome and hormone replacement therapy. BMJ (Clinical research ed.). Feb 8 1992;304(6823):382.
Hammer HB, Haavardsholm EA, Kvien TK. Ultrasonographic measurement of the median nerve in patients with rheumatoid arthritis without symptoms or signs of carpal tunnel syndrome. Annals of the rheumatic diseases. Jun 2007;66(6):825-827.
Hammer HB, Hovden IA, Haavardsholm EA, Kvien TK. Ultrasonography shows increased cross-sectional area of the median nerve in patients with arthritis and carpal tunnel syndrome. Rheumatology (Oxford, England). May 2006;45(5):584-588.
Hassan Z, Mullins RF, Alam B, Mian MAH. Carpal tunnel syndrome following burns. Annals Burn Fire Disasters 2008;XXI:153-155.
Hassanpour SE, Gousheh J. Mycobacterium tuberculosis-induced carpal tunnel syndrome: Management and follow-up evaluation. J Hand Surgery 2006;31A:575-579.
Hemminger A, Wills BK. Vitamin B6 Toxicity. StatPearls. 2026.
Hirata H, Nagakura T, Tsujii M, Morita A, Fujisawa K, Uchida A. The relationship of VEGF and PGE2 expression to extracellar matrix remodeling of the tenosynovium in the carpal tunnel syndrome. J Pathology 2004;204:605-612.
Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. Jul 2011;96(7):1911-30. doi:10.1210/jc.2011-0385. https://www.ncbi.nlm.nih.gov/pubmed/21646368
Huisstede BM, Hoogvliet P, Randsdorp MS, Glerum S, Van Middelkoop M, Koes BW. Carpal tunnel syndrome. Part 1. Effectiveness of nonsurgical treatments - a systemic review. Arch Phys Med Rehabil 2010;91:981-1004.
Huisstede BM, Randsdrop MS, Coert JH, Glerum S. Van Middelkoop M, Koes BW. Carpal tunnel syndrome. Part 2. Effectiveness of surgical treatments - a systematic review. Arch Phys Med Rehabil 2010;91:1005-1024.
Ibrahim I, Khan WS, Goddard N, Smitham P. Carpal tunnel syndrome: a review of the recent literature. The open orthopaedics journal. 2012;6:69-76.
Jain JB, Higgins LD, Losina E, Collins J, Blazar DS, Katz JN. Epidemiology of upper extremity disorders in the United States. BMC Musculoskeletal Disorders 2014;15:4.
Jungert A, McNulty H, Hoey L, et al. Riboflavin Is an Important Determinant of Vitamin B-6 Status in Healthy Adults. J Nutr. Oct 12 2020;150(10):2699-2706. doi:10.1093/jn/nxaa225. https://www.sciencedirect.com/science/article/pii/S0022316622023392?via%3Dihub
Kaplan Y, Kurt SG, Karaer H. Carpal tunnel syndrome in postmenopausal women. Journal of the neurological sciences. Jul 15 2008;270(1-2):77-81.
Karadag O, Kalyoncu U, Akdogan A, Karadag YS, Bilgen SA, Ozbakir S, . . . Calguneri M. Sonographic assessment of carpal tunnel syndrome in rheumatoid arthritis: prevalence and correlation with disease activity. Rheumatology international. Aug 2012;32(8):2313-2319.
Kececi H, Degirmenci Y. Hormone replacement therapy in hypothyroidism and nerve conduction study. Clinical Neurophysiology 2006;36(2):79-93.
Keir PJ, Bach JM, Hudes M, Rempel DM. Guidelines for wrist posture based on carpal tunnel pressure thresholds. Human Factors 2007;49:88-99.
Keniston RC, Nathan PA, Leklem JE, Lockwood RS. Vitamin B6, vitamin C, and carpal tunnel syndrome. J Occup Environ Med 1997;39:949-959.
Kerasnoudis A. Could sonographically guided percutaneous needle release of the carpal tunnel also play an important role in the treatment of recurrent carpal tunnel syndrome? Journal of ultrasound in medicine: official journal of the American Institute of Ultrasound in Medicine. Dec 2012;31(12):2048-2049; author reply 2049.
Khosrawi S, Moghtaderi A, Haghighat S. Acupuncture in treatment of carpal tunnel syndrome: A randomized controlled trial study.J Res Med Sci 2012;17:1-7.
Kilot M. Carpal Tunnel Syndrome. First Consult. Clinical Key webpage. Available at: www.clinicalkey.com. Last updated 6/19/2013. Accessed 3/4/2014
Kim JK, Hann HJ, Kim MJ, Kim JS. The expression of estrogen receptors in the tenosynovium of postmenopausal women with idiopathic carpal tunnel syndrome. Journal of orthopaedic research: official publication of the Orthopaedic Research Society. Nov 2010;28(11):1469-1474.
Kim JK, Koh YD, Kim JS, Hann HJ, Kim MJ. Oxidative stress in subsynovial connective tissue of idiopathic carpal tunnel syndrome. J Orthoped Res 2010;28:1463-1468.
Ko GD, Nowacki NB, Arseneau L, Eitel M, Hum A. Omega-3 fatty acids for neuropathic pain: Case series. Clin J Pain 2010;26:168-172.
Kostopoulos D. Treatment of carpal tunnel syndrome: a review of the non-surgical approaches with emphasis in neural mobilization. Available at http://somasimple.com/pdf_files/carpal_tunel.pdf Accessed 08/19/2014. Journal of Bodywork and Movement Therapies. 2004;8(1):2-8.
Kurt S, Kisacik B, Kaplan Y, Yildirim B, Etikan I, Karaer H. Obesity and carpal tunnel syndrome: is there a causal relationship? European neurology. 2008;59(5):253-257.
Kwon JY, Ko K, Sohn YB, Kim SJ, Park SW, Kim SH, . . . Jin DK. High prevalence of carpal tunnel syndrome in children with mucopolysaccharidosis type II (Hunter syndrome). American journal of medical genetics. Part A. Jun 2011;155a(6):1329-1335.
LeBlanc KE, Cestia W. Carpal tunnel syndrome. Am Fam Physician 2011;83:952-958.
Lederman RJ. Focal peripheral neuropathies in instrumental musicians.Phys Med Rehabil Clin N Am 2006;761-769.
Leduc A, Perrot P, Truffandier MV, Bellier-Waast F, Duteille F. [Carpal tunnel syndrome in children. About 10 clinical cases]. Annales de chirurgie plastique et esthetique. Jun 2014;59(3):155-160.
Lewanska M, Wagrowska-Koski E, Walusiak-Skorupa J. [Etiological factors for developing carpal tunnel syndrome in people who work with computers]. Medycyna pracy. 2013;64(1):37-45.
Madenci E, Altindag O, Koca I, Yilmaz M, Gur A. Reliability and efficacy of the new massage technique on the treatment in the patients with carpal tunnel syndrome. Rheumatology International 2012;32:3171-3179.
Marshall S, Tardif G, Ashworth N. Local corticosteroid injection for carpal tunnel syndrome. The Cochrane database of systematic reviews. 2007(2):Cd001554.
Mattioli S, Baldasseroni A, Curti S, Cooke RM, Bena A, de Giacomi G, . . . Violante FS. Incidence rates of in-hospital carpal tunnel syndrome in the general population and possible associations with marital status. BMC public health. 2008;8:374.
Mayo Clinic. Carpal Tunnel Syndrome: Causes. Available at: http://www.mayoclinic.org/diseases-conditions/carpal-tunnel-syndrome/basics/causes/con-20030332. 4/2/2014. Accessed 08/15/2014.
McDonagh C, Alexander M, Kane D. The role of ultrasound in the diagnosis and management of carpal tunnel syndrome: a new paradigm. Rheumatology (Oxford, England). Aug 12 2014.
McShane JM, Slaff S, Gold JE, Nazarian LN. Sonographically guided percutaneous needle release of the carpal tunnel for treatment of carpal tunnel syndrome: preliminary report. Journal of ultrasound in medicine: official journal of the American Institute of Ultrasound in Medicine. Sep 2012;31(9):1341-1349.
Mediouni Z, De Roquemaurel A, Dumontier C, Becour B, Garrabe H, Roquelaure Y, Descatha A. Is carpal tunnel syndrome related to computer exposure at work? A review and meta-analysis. J Occup Environ Med 2014;56:204-208.
Memeo A, Loiero M. Thioctic acid and acetyl-L-carnitine in the treatment of sciatic pain caused by a herniated disc: a randomized, double-blind, comparative study. Clinical drug investigation. 2008;28(8):495-500.
Mieog JS, Morden JP, Bliss JM, Coombes RC, van de Velde CJ. Carpal tunnel syndrome and musculoskeletal symptoms in postmenopausal women with early breast cancer treated with exemestane or tamoxifen after 2-3 years of tamoxifen: a retrospective analysis of the Intergroup Exemestane Study. The lancet oncology. Apr 2012;13(4):420-432.
Mijnhout GS, Alkhalaf A, Kleefstra N, Bilo HJ. Alpha lipoic acid: a new treatment for neuropathic pain in patients with diabetes? The Netherlands journal of medicine. Apr 2010;68(4):158-62. https://www.ncbi.nlm.nih.gov/pubmed/20421656
Moghtaderi AR, Jazayeri SM, Azizi S. EMLA cream for carpal tunnel syndrome: how it compares with steroid injection. Electomyogr Clin Neurophysiol 2009;49:287-289.
Mondelli M, Rossi S, Monti E, Aprile I, Caliandro P, Pazzaglia C, . . . Padua L. Long term follow-up of carpal tunnel syndrome during pregnancy: a cohort study and review of the literature. Electromyography and clinical neurophysiology. Sep 2007;47(6):259-271.
Moraska A, Chandler C, Edmison-Schaetzel A, Franklin G, Calenda EL, Enebo B. Comparison of a targeted and general massage protocol on strength, function, and symptoms associated with carpal tunnel syndrome: A randomized pilot study. Journal of Alternative and Complimentary Medicine 2008;14:259-267.
Naeser MA, Hahn KAK, Lieberman BE, Branco KF. Carpal tunnel syndrome pain treated with low-level laser and microamperes transcutaneous electric nerve stimulation: A controlled study. Arch Phys Med Rehabil 2002;83:978-988.
Nakamichi K, Tachibana S, Yamamoto S, Ida M. Percutaneous carpal tunnel release compared with mini-open release using ultrasonographic guidance for both techniques. The Journal of hand surgery. Mar 2010;35(3):437-445.
Nalamachu S, Crockett RS, Gammaitoni AR, Gould EM. A comparison of lidocaine patch 5% vs naproxen 500 mg twice daily for the relief of pain associated with carpal tunnel syndrome: A 6-week, randomized, parallel-group study. Med Gen Med 2006;8:33
Nathan PA, Wilcox A, Emerick PS, Meadows KD, McCormack AL. Effects of an aerobic exercise program on median nerve conduction and symptoms associated with carpal tunnel syndrome. J Occup Environ Med 2001;43:840-843.
Nishihori T, Choi J, DiGiovanna MP, Thomson JG, Kohler PC, McGurn J, et al. Carpal tunnel syndrome associated with the use of aromatase inhibitors in breast cancer. Clinical Breast Cancer 2008;8(4):362-365.
O’Connor D, Marshall S, Massy-Westropp N, Pitt V. Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome. Cochrane Database of Systematic Reviews 2003, Issue 1. Art. No.:CD003219. DOI 10.1002/14651858.CD003219
Onder B, Yalcin E, Selcuk B, Kurtaran A, Akyuz M. Carpal tunnel syndrome and metabolic syndrome co-occurrence. Rheumatology international. Mar 2013;33(3):583-586.
Osiri M, Welch V, Brosseau L, Shea B, McGowan J, Tugwell P, Wells G. Transcutaneous electrical nerve stimulation for knee osteoarthritis. The Cochrane database of systematic reviews. 2000(4):Cd002823.
Osterman M, Ilyas AM, Matzon JL. Carpal tunnel syndrome in pregnancy. Orthoped Clin N Am 2012;43:515-520.
Ozturk N, Erin N, Tuzuner S. Changes in tissue substance P levels in patients with carpal tunnel syndrome. Neurosurgery. Dec 2010;67(6):1655-1660; discussion 1660-1651.
Padua L, Di Pasquale A, Pazzaglia C, Liotti GA, Librante A, Mondelli M. Systematic review of pregnancy-related carpal tunnel syndrome. Muscle Nerve 2010;42:697-703.
Paecharoen S, Wongsuphasawat K, Tantiyavarong P. Efficacy of Omega-3 Farry Acids in the Treatment of Carpal Tunnel Syndrome: A Randomized Double-Blind Controlled Trial. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2020;103(2): 106-114. https://www.cabidigitallibrary.org/doi/full/10.5555/20203413189
Page MJ, Massy-Westropp N, O’Connor D, Pitt V. Splinting for carpal tunnel syndrome. Cochrane Database Syst Rev. 2012; 7:CDE010003. doi: 10.1002/14651858.CD010003.
Pajardi G, Bortot P, Ponti V, Novelli C. Clinical usefulness of oral supplements with alpa-lipoic acid, curcumin phytosome, and B-group vitamins in patients with carpal tunnel syndrome undergoing surgical treatment. Evidence Based Compliment Altern Med 2014: 891310. http://dx.doi.org/10.1155/2014/891310
Palmer KT. Carpal tunnel syndrome: The role of occupational factors. Best Practice & Research Clinical Rheumatology 2011;25:15-29.
Palumbo CF, Szabo RM, Olmsted SL. The effects of hypothyroidism and thyroid replacement on the development of carpal tunnel syndrome. J Hang Surg 2000;25A: 734-739.
Panagariya A, Sharma AK. A preliminary trial of serratiopeptidase in patients with carpal tunnel syndrome. J Assoc Physicians India 1999;47:1170-1172.
Pandey A, Usman K, Reddy H, Gutch M, Jain N, Qidwai S. Prevalence of hand disorders in type 2 diabetes mellitus and its correlation with microvascular complications. Annals of medical and health sciences research. Jul 2013;3(3):349-354.
Papanas N, Maltezos E. The diabetic hand: a forgotten complication? J Diabetes Complications 2010;24:154-162
Parisi S, Ditto MC, Borrelli R, Fusaro E. Efficacy of a fixed combination of palmitoylethanolamide and acetyl-l-carnitine (PEA+ALC FC) in the treatment of neuropathies secondary to rheumatic diseases. Minerva Med. Aug 2021;112(4):492-499. doi:10.23736/S0026-4806.21.07486-3. https://www.ncbi.nlm.nih.gov/pubmed/34056884
Park JH, Kim SN, Han SM, Cheon KY, Han SW, Kim JY, et al. Carotid intima-media thickness in patients with carpal tunnel syndrome. J Ultrasound Med 2013;32:1753-1757.
Pascual E, Giner V, Arostegui A, Conill J, Ruiz MT, Pico A. Higher incidence of carpal tunnel syndrome in oophorectomized women. British journal of rheumatology. Feb 1991;30(1):60-62.
Passiatore M, Perna A, De-Vitis R, Taccardo G. The Use of Alfa-Lipoic Acid-R (ALA-R) in Patients with Mild-Moderate Carpal Tunnel Syndrome: A Randomised Controlled Open Label Prospective Study. Malays Orthop J. Mar 2020;14(1):1-6. doi:10.5704/MOJ.2003.001. https://www.ncbi.nlm.nih.gov/pubmed/32296475
Plastino M, Fava A, Carmela C, De Bartolo M, Ermio C, Cristiano D, . . . Bosco D. Insulin resistance increases risk of carpal tunnel syndrome: a case-control study. Journal of the peripheral nervous system: JPNS. Sep 2011;16(3):186-190.
Potulska-Chromik A, Lipowska M, Gawel M, Ryniewicz B, Maj E, Kostera-Pruszczyk A. Carpal tunnel syndrome in children. Journal of child neurology. Feb 2014;29(2):227-231.
Proctor ML, Smith CA, Farquhar CM, Stones RW. Transcutaneous electrical nerve stimulation and acupuncture for primary dysmenorrhoea. The Cochrane database of systematic reviews. 2002(1):Cd002123.
Raman SR, Al-Halabi B, Hamdan E, Landry MD. Prevalence and risk factors associated with self-reported carpal tunnel syndrome (CTS) among office workers in Kuwait. BMC research notes. 2012;5:289.
Redmond CL, Bain GI, Laslett LL, McNeil JD. Hand syndromes associated with diabetes: impairments and obesity predict disability. The Journal of rheumatology. Dec 2009;36(12):2766-2771.
Reljanovic M, Reichel G, Rett K, Lobisch M, Schuette K, Moller W, . . . Mehnert H. Treatment of diabetic polyneuropathy with the antioxidant thioctic acid (alpha-lipoic acid): a two year multicenter randomized double-blind placebo-controlled trial (ALADIN II). Alpha Lipoic Acid in Diabetic Neuropathy. Free radical research. Sep 1999;31(3):171-179.
Rempel DM, Keir PJ, Bach JM. Effect of wrist posture on carpal tunnel pressure when typing. J Orthop Res 2008;26:1269-1273.
Robb KA, Bennett MI, Johnson MI, Simpson KJ, Oxberry SG. Transcutaneous electric nerve stimulation (TENS) for cancer pain in adults. The Cochrane database of systematic reviews. 2008(3):Cd006276.
Rojo-Manaute JM, Capa-Grasa A, Rodriguez-Maruri GE, Moran LM, Martinez MV, Martin JV. Ultra-minimally invasive sonographically guided carpal tunnel release: anatomic study of a new technique. Journal of ultrasound in medicine: official journal of the American Institute of Ultrasound in Medicine. Jan 2013;32(1):131-142.
Saçmaci H, Tanik N, Balbaloğlu Ö, Aktürk T, Inan LE. Electrophysiological evaluation of carpal tunnel syndrome female patients after vitamin D replacement. Arquivos de neuro-psiquiatria. Apr 2020;78(4):224-229. doi:10.1590/0004-282x20190193. https://www.scielo.br/j/anp/a/BPBsCNQB6HtHhqqQRvKPQBq/?lang=en&format=pdf
Salinthone S, Yadav V, Schillace RV, Bourdette DN, Carr DW. Lipoic acid attenuates inflammation via cAMP and protein kinase A signaling. PloS one. 2010;5(9).
Samant PD, Sane RM. Evaluation of Functional and Symptomatic Outcomes After Vitamin D(3) Administration in Carpal Tunnel Syndrome With Hypovitaminosis D. Hand (N Y). Nov 2022;17(6):1065-1069. doi:10.1177/1558944720988130. https://pmc.ncbi.nlm.nih.gov/articles/PMC9608297/
Sbruzzi G, Silveira SA, Silva DV, Coronel CC, Plentz RD. Transcutaneous electrical nerve stimulation after thoracic surgery: systematic review and meta-analysis of 11 randomized trials. Revista brasileira de cirurgia cardiovascular: orgao oficial da Sociedade Brasileira de Cirurgia Cardiovascular. Jan-Mar 2012;27(1):75-87.
Schreiber AL, Sucher BM, Nazarian LN. Two novel nonsurgical treatments of carpal tunnel syndrome. Physical medicine and rehabilitation clinics of North America. May 2014;25(2):249-264.
Seror P, Seror R. Prevalence of obesity and obesity as a risk factor in patients with severe median nerve lesion at the wrist. Joint, bone, spine: revue du rhumatisme. Dec 2013;80(6):632-637.
Sestak I, Sapunar F, Cuzick J. Aromatase inhibitor-induced carpal tunnel syndrome: results from the ATAC trial. J Clinical Oncology 2009;27:4961-4965.
Shi Q, MacDermid JC. Is surgical intervention more effective than non-surgical treatment for carpal tunnel syndrome? A systematic review. Journal of orthopaedic surgery and research. 2011;6:17.
Shi Y, Shi Y, Jie R, He J, Luo Z, Li J. Vitamin D: The crucial neuroprotective factor for nerve cells. Neuroscience. Nov 12 2024;560:272-285. doi:10.1016/j.neuroscience.2024.09.042.
Shiri R, Heliovaara M, Moilanen L, Viikari J, Liira H, Viikari-Juntura E. Associations of cardiovascular risk factors, carotid intima-media thickness and manifest atherosclerotic vascular disease with carpal tunnel syndrome. BMC musculoskeletal disorders. 2011;12:80.
Shooshtari SM, Badiee V, Taghizadeh SH, Nematollahi AH, Amanollahi AH, Grami MT. The effects of low level laser in clinical outcome and neurophysiological results of carpal tunnel syndrome. Electromyography and clinical neurophysiology. Jun-Jul 2008;48(5):229-231.
Simon H, Zieve D. University of Maryland Medical Center website. Carpal tunnel syndrome. Available at: http://umm.edu/health/medical/reports/articles/carpal-tunnel-syndrome. 5/26/2012. Accessed 4/24/2014.
Siu G, Jaffe JD, Rafique M, Weinik MM. Osteopathic manipulative medicine for carpal tunnel syndrome. The Journal of the American Osteopathic Association. Mar 2012;112(3):127-139.
Spahn G, Wollny J, Hartmann B, Schiele R, Hofmann GO. [Metaanalysis for the evaluation of risk factors for carpal tunnel syndrome (CTS) Part I. General factors]. Zeitschrift fur Orthopadie und Unfallchirurgie. Oct 2012;150(5):503-515.
Stevens JC, Beard CM, O'Fallon WM, Kurland LT. Conditions associated with carpal tunnel syndrome. Mayo Clinic proceedings. Mayo Clinic. Jun 1992;67(6):541-548.
Sucher BM, Hinrichs RN. Manipulative treatment of carpal tunnel syndrome: biomechanical and osteopathic intervention to increase the length of the transverse carpal ligament. The Journal of the American Osteopathic Association. Dec 1998;98(12):679-686.
Sucher BM. Osteopathic manipulative medicine for carpal tunnel syndrome. The Journal of the American Osteopathic Association. Jun 2012;112(6):383-384; author reply 384.
Sugimoto K, Yasujima M, Yagihashi S. Role of advanced glycation end products in diabetic neuropathy. Current pharmaceutical design. 2008;14(10):953-961.
Szabo RM, Slater RR, Jr., Farver TB, Stanton DB, Sharman WK. The value of diagnostic testing in carpal tunnel syndrome. The Journal of hand surgery. Jul 1999;24(4):704-714.
Talebi M, Andalib S, Bakhti S, Ayromlou H, Aghili A, Talebi A. Effect of vitamin B6 on clinical symptoms and electrodiagnostic results of patients with carpal tunnel syndrome. Advanced Pharmaceutical Bulletin 2013;3:283-288.
Talmor M, Patel MP, Spann MD, Barden C, Specht M, McLean A, et al. COX-2 up-regulation in idiopathic carpal tunnel syndrome. Plast Reconstr Surg 2003;112:1807-1817.
Tarallo M, Fino P, Sorvillo V, Parisi P, Scuderi N. Comparative analysis between minimal access versus traditional accesses in carpal tunnel syndrome: A prospective randomized study. J Plastic Reconstructive and Aesthetic Surgery 2014;67:237-243.
Teichert J, Hermann R, Ruus P, Preiss R. Plasma kinetics, metabolism, and urinary excretion of alpha-lipoic acid following oral administration in healthy volunteers. J Clin Pharmacol. Nov 2003;43(11):1257-67. doi:10.1177/0091270003258654. https://accp1.onlinelibrary.wiley.com/doi/abs/10.1177/0091270003258654?sid=nlm%3Apubmed
Thomsen JF, Gerr F, Atroshi I. Carpal tunnel syndrome and the use of computer mouse and keyboard: a systematic review. BMC musculoskeletal disorders. 2008;9:134.
Tseng CH, Liao CC, Kuo CM, Sung FC, Hsieh DP, Tsai CH. Medical and non-medical correlates of carpal tunnel syndrome in a Taiwan cohort of one million. European journal of neurology: the official journal of the European Federation of Neurological Societies. Jan 2012;19(1):91-97.
Tucci MA, Berbieri RA, Freeland AE. Biochemical and histological analysis of the flexor tenosynovium in patients with carpal tunnel syndrome. Biomed Sci Instrum 1997;33: 246-251.
Uchida R, Okamoto H, Ikuta N, Terao K, Hirota T. Enantioselective Pharmacokinetics of α-Lipoic Acid in Rats. International journal of molecular sciences. Sep 21 2015;16(9):22781-94. doi:10.3390/ijms160922781. https://pmc.ncbi.nlm.nih.gov/articles/PMC4613335/
Van Meir N, De Smet L. Carpal tunnel syndrome among children. Acta Orthopaedica Belgica 2003;69:387-395.
Vasiliadis HS, Georgoulas P, Shrier I, Salanti G, Scholten RJ. Endoscopic release for carpal tunnel syndrome. The Cochrane database of systematic reviews. 2014;1:Cd008265.
Visser LH, Ngo Q, Groeneweg SJ, Brekelmans G. Long term effect of local corticosteroid injection for carpal tunnel syndrome: a relation with electrodiagnostic severity. Clinical neurophysiology: official journal of the International Federation of Clinical Neurophysiology. Apr 2012;123(4):838-841.
Von Glehn F, Damasceno A, Miotto N, Naseri EP, Costallat LTL, Franca MC, et al. Carpal tunnel syndrome with paracoccidioidomycosis. Emerging Infect Dis 2012;18: 1390-1392.
Wallace WA. Injection with methylprednisolone for carpal tunnel syndrome. Local steroid injections only reduce inflammation temporarily. BMJ (Clinical research ed.). Mar 4 2000;320(7235):645-646.
Walter N, Bourgois P, Margarita Loinaz H, Schillinger D. Social context of work injury among undocumented day laborers in San Francisco. Journal of general internal medicine. Mar 2002;17(3):221-229.
White K, Kim T, Neufeld JA. Clinical assessment and treatment of carpal tunnel syndrome in the mucopolysaccharidoses. J Ped Rehab Med 2010;3:57-62.
Wikimedia Commons. Images. Carpal tunnels page: Carpal Tunnel Syndrome. Available at: http://commons.wikimedia.org/wiki/File:Carpal_Tunnel_Syndrome.png. Last updated 2/21/2014. Accessed 4/24/2014.
Wilson RJ, Watson JT, Lee DH. Nerve entrapment syndromes in musicians. Clinical Anatomy 2014; In Press
Wong SM, Hui ACF, Tang A, Ho PC, Hung LK, Wong KS, et al. Local versus systemic corticosteroids in the treatment of carpal tunnel syndrome. Neurology 2001;56:1565-1567.
Yagci I, Elmas O, Akcan E, Ustun I, Gunduz OH, Guven Z. Comparison of splinting and splinting plus low-level laser therapy in idiopathic carpal tunnel syndrome. Clinical rheumatology. Sep 2009;28(9):1059-1065.
Yildirim A, Bulut HT, Ekmekci B, Dost Surucu G, Karabiber M. Use of diffusion tensor imaging for non-surgical treatments of carpal tunnel syndrome. Muscle Nerve 2014; In Press Doi 10.1002/mus.24236.
Xu ZZ, Zhang L, Liu T, et al. Resolvins RvE1 and RvD1 attenuate inflammatory pain via central and peripheral actions. Nat Med. May 2010;16(5):592-7, 1p following 597. doi:10.1038/nm.2123. https://www.nature.com/articles/nm.2123
Zhang Y, Han P, Wu N, He B, Lu Y, Li S, . . . Li Y. Amelioration of lipid abnormalities by alpha-lipoic acid through antioxidative and anti-inflammatory effects. Obesity (Silver Spring, Md.). Aug 2011;19(8):1647-1653.
Ziegler D, Ametov A, Barinov A, Dyck PJ, Gurieva I, Low PA, . . . Samigullin R. Oral treatment with alpha-lipoic acid improves symptomatic diabetic polyneuropathy: the SYDNEY 2 trial. Diabetes care. Nov 2006;29(11):2365-2370.
Ziegler D, Nowak H, Kempler P, Vargha P, Low PA. Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a meta-analysis. Diabetic medicine: a journal of the British Diabetic Association. Feb 2004;21(2):114-121.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun