Life Extension Magazine.

Danger Of Omitting Blood Tests
The ApoB blood test is an often-overlooked indicator of cardiovascular risk. A new study found testing ApoB and CRP together can better predict atherosclerotic disease.
Scientifically reviewed by: Gary Gonzalez, MD, in April 2026. Written by: Chancellor Faloon.
A 2024 large-scale analysis of blood test orders from millions of physicians identified a startling finding:
The vast majority are not testing critical marker of cardiovascular disease risk and status.
The data revealed that, over a one-year period (2019), 99% of blood tests that included lipid panel components omitted important biomarkers like apolipoprotein-B (ApoB).1
Elevated ApoB is an important factor in the formation of atherosclerotic plaques in the coronary arteries,1 which increases the risk of myocardial infarction (MI) aka “heart attack.”2
A big reason why many physicians do not order ApoB testing is because conventional wisdom suggests that risk assessment of MI can be accurately inferred from LDL-cholesterol (LDL-C) levels.1
Emerging evidence, however, suggests that ApoB provides additional predictive risk beyond LDL-C.1,3,4
One study published in the Journal of the American College of Cardiology demonstrated a great degree of unanticipated cardiovascular risk in those with elevated ApoB levels.
Men and women with the most unexpected ApoB levels, based on their LDL-C results, had a 52% and 75% increased risk of atherosclerotic heart disease, respectively, compared to those who had the most expected levels.3
Failure to measure ApoB in certain at-risk populations may therefore contribute to a substantial number of preventable deaths.
Given the prevalence of atherosclerotic coronary artery disease, ApoB, along with other blood biomarkers in cardiovascular risk assessment, should not be omitted.
A Bigger Picture of Cardiovascular Health Status
An estimated 38% of insured Americans had testing for any lipid panel component in the year 2019.
Deep analysis into what these lipid panels consisted of revealed that two important cardiovascular risk factors, ApoB and Lipoprotein (a) or Lp(a), made up less than 1% of these lipid tests.1This suggests physicians are underusing tools that could more accurately assess heart attack risk for many patients.
Conventional routine cholesterol testing with a general CBC/Chem panel may not be enough for everyone, and with a rapidly aging population, there is an urgent need for better testing.
Life Extension® readers know about LDL, but many may not fully understand what an LDL-C test is.
An LDL-C test calculates the total amount of cholesterol carried by an LDL particle.
What LDL-C tests do not measure is the total amount of atherogenic particles; this is what an ApoB test is for.
ApoB levels reflect the total number of high-risk, circulating, artery-clogging particles.5
ApoB-containing particles can enter the wall of arteries and get stuck, especially in areas where the artery wall is vulnerable from chronic inflammation.
This trapping is a critical step in the development and progression of atherosclerosis.6
The more ApoB-containing particles are present, the more likely they are to accumulate in the artery wall.
This leads to the formation of plaques which can grow, become inflamed, and eventually block blood flow, causing heart attacks or strokes. The other test often omitted from lipid panels is Lp(a), which measures a “special” LDL cholesterol particle that makes plaque buildup and clotting more likely. It’s mostly unaffected by lifestyle but can provide additional assessment of cardiovascular risk.
Unlike other blood markers that often worsen with age and poor lifestyles, elevated Lp(a) is a genetically programmed risk factor that typically only needs to be tested once to identify those at increased cardio-vascular risk caused by elevated Lp(a).7
Why You Should Test ApoB
Many physicians undervalue ApoB testing, assuming LDL-C alone can predict its results. Emerging evidence shows that groups with metabolic disorders such as obesity, diabetes, or dyslipidemia, are more likely to have higher-than-expected ApoB levels.5
The Risk of Atherosclerotic Coronary Artery Disease with Excess ApoB
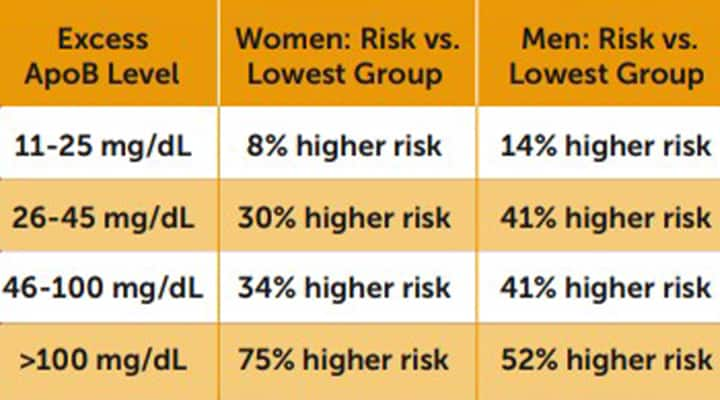
The table above depicts the group risk differences of atherosclerotic coronary artery disease for people with excess ApoB levels, compared to those below an excess of 11 mg/dL, in the Journal of the American College of Cardiology published study.3
In a 2024 study published in the Journal of the American College of Cardiology, approximately 100,000 people were followed for nearly 10 years, and researchers assessed the effects of “excess ApoB,” defined as measured ApoB minus the level expected based on the observed LDL-C.3

The results showed that those with excess ApoB greater than 11 mg/dL had greater risks of atherosclerotic coronary artery disease.
Men and women with more than 100 mg/dL of excess ApoB had a 52% and a 75% higher risk, respectively, compared with those whose excess ApoB was below 11 mg/dL.
Higher excess ApoB levels were associated with a progressive increase in current smoking prevalence, systolic blood pressure, BMI, and diabetes.
These results suggest that if a physician omits testing ApoB in a patient with these characteristics, then they may be ignoring a critical signal of a looming heart attack if their LDL-C results come back normal.
Even Mild CRP Elevations Predict Major Cardiovascular Events
C-reactive protein (CRP) is a marker of systemic inflammation, yet it has been historically under-utilized in cardiovascular prevention care.
What ApoB Levels Are Recommended?
According to The National Lipid Association, ApoB should be below 90 mg/dL for generally healthy people and below 60 mg/dL for those with a high risk of cardiovascular morbidity and mortality.11
Some argue that ApoB levels should be even lower.
In one large randomized-controlled trial, about 28,000 people with cardiovascular disease who were receiving statin treatment were randomized to receive an aggressive form of lipid-lowering therapy with a PCSK9 inhibitor or a placebo.12 Multiple sources have confirmed that those who received the treatment had their median ApoB levels sink below 50 mg/dL.11,13 This demonstrated additional cardiovascular risk protection compared to placebo. However, it should be noted that this clinical trial was not designed to assess differing benefits based on ApoB ranges.
ApoB levels that are too low may also increase the risk of mortality.14
In 2025 The American College of Cardiology finally recommended CRP testing for both primary and secondary prevention of cardiovascular disease.8,9
A new study found that even mild elevations in CRP were associated with greater risk of major adverse cardiovascular events (MACE).9
Over 12,500 healthy American women were followed for 30 years and 973 MACE events were recorded. None of the women had high cardiovascular risk factors such as hypertension, dyslipidemia, diabetes mellitus, and smoking.
Women who experienced a MACE event had a significantly higher average baseline CRP (2.22 mg/L) compared with those who did not (1.5 mg/L).
A CRP level above 3 mg/L was associated with:

- 77% higher risk of coronary heart disease,
- 39% higher risk of ischemic stroke, and
- 52% higher risk of total cardiovascular events.
Optimal CRP levels are under 1.0 mg/L, but many individuals have higher concentrations, often without knowing it.
Why You Should Test ApoB and CRP Together
While multiple studies have shown that there is independent value in testing ApoB and CRP,3,6,7 a new study found their combination was a better predictor of atherosclerotic cardiovascular disease, compared to a panel of standard and specialized lipid risk factors.10
Approximately 270,000 people in the UK Biobank cohort, with an average age of 56, were followed for up to 15 years. The researchers measured the following at baseline:
- LDL-C,
- Non-HDL-C,
- Estimated small dense LDL,
- Estimated low-density lipoprotein triglyceride,
- Apolipoprotein B, and
- C-reactive protein.
All tests predicted atherosclerotic cardiovascular disease, however an ApoB >130 mg/dL combined with CRP > 2 mg/L resulted in a 69% increased risk of a major adverse cardiovascular event, which was more predictive than all other biomarkers tested.
To give the best prediction of cardiovascular disease risk and mortality, we suggest that all these biomarkers be evaluated.
Potential Pharmacological Therapies to Lower Stubborn Lp(a) in Development
Approximately 20% of people are at a higher risk of cardiovascular disease due to high Lp(a), which is primarily genetically determined.15
The explanation that doctors give their patients for why they typically do not test for Lp(a) is that there is no pharmaceutical treatment.16
That may soon change. A meta-analysis of 41 randomized controlled trials found that PCSK9 inhibitors lowered lipoprotein(a) Lp(a) levels by an average of 27% compared to another lipid-lowering drug, ezetimibe.13
There are now five experimental drugs demonstrating substantial Lp(a) reductions in phase II clinical trials, with large phase III trials underway or set to begin.17
The furthest along is pelacarsen, for which we can expect to see phase III results soon.18 However, in a phase II study, olpasiran injected every 12 weeks resulted in reductions of Lp(a) exceeding 70% compared to the placebo group.19
While the eventual cost of these therapies is still unknown, their approval could mark the first effective treatment options for patients with persistently high Lp(a).
Summary
New research sheds light on the importance of ApoB testing, especially for those with underlying metabolic disorders.
However, an analysis of blood testing found that 99% of tests that included lipid panel components in 2019 omitted this test.
Researchers predict that as the atherogenic impact of biomarkers like ApoB become more widely known, physicians will include them in routine blood test panels.
We at Life Extension® implore our readers to test these biomarkers to provide a more detailed picture of their cardiovascular health.
Ask your doctor to include these markers at your next cholesterol test. If unable to get them through your doctor, Life Extension has included these markers in our extremely popular Male and Female panels.
If you have any questions on the scientific content of this article, please call a Life Extension Wellness Specialist at 1-866-864-3027.
References
- Murdock DJ, Moll K, Sanchez RJ, et al. Low prevalence of testing for apolipoprotein B and lipoprotein (a) in the real world. Am J Prev Cardiol. 2024 Sep;19:100721.
- Wang KL, Balmforth C, Meah MN, et al. Coronary Atherosclerotic Plaque Activity and Risk of Myocardial Infarction. J Am Coll Cardiol. 2024 Jun 4;83(22):2135-44.
- Johannesen CDL, Langsted A, Nordestgaard BG, et al. Excess Apolipoprotein B and Cardiovascular Risk in Women and Men. J Am Coll Cardiol. 2024 Jun 11;83(23):2262-73.
- Cole J, Otvos JD, Remaley AT. A Translational Tool to Facilitate Use of Apolipoprotein B for Clinical Decision-Making. Clin Chem. 2023 Jan 4;69(1):41-7.
- Galimberti F, Casula M, Olmastroni E. Apolipoprotein B compared with low-density lipoprotein cholesterol in the atherosclerotic cardiovascular diseases risk assessment. Pharmacol Res. 2023 Sep;195:106873.
- Boren J, Packard CJ, Binder CJ. Apolipoprotein B-containing lipoproteins in atherogenesis. Nat Rev Cardiol. 2025 Jun;22(6):399-413.
- Bjornson E, Adiels M, Taskinen MR, et al. Lipoprotein(a) Is Markedly More Atherogenic Than LDL: An Apolipoprotein B-Based Genetic Analysis. J Am Coll Cardiol. 2024 Jan 23;83(3):385-95.
- Mensah GA, Arnold N, Prabhu SD, et al. Inflammation and Cardiovascular Disease: 2025 ACC Scientific Statement: A Report of the American College of Cardiology. J Am Coll Cardiol. 2025 Sep 29.
- Ridker PM, Figtree GA, Moorthy MV, et al. C-reactive protein and cardiovascular risk among women with no standard modifiable risk factors: evaluating the ‘SMuRF-less but inflamed’. Eur Heart J. 2026 Jan 16;47(3):306-14.
- Zubiran R, Sampson M, Remaley A. Abstract Th0013: Apolipoprotein B and C-Reactive Protein Identifies High Cardiovascular Risk More Effectively Than Traditional Lipid Biomarkers. Arteriosclerosis, Thrombosis, and Vascular Biology. 2025 2025/04/01;45(Suppl_1):ATh0013-ATh.
- Soffer DE, Marston NA, Maki KC, et al. Role of apolipoprotein B in the clinical management of cardiovascular risk in adults: An Expert Clinical Consensus from the National Lipid Association. J Clin Lipidol. 2024 Sep-Oct;18(5):e647-e63.
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N Engl J Med. 2017 May 4;376(18):1713-22.
- Rosenblit PD. Lowering Targeted Atherogenic Lipoprotein Cholesterol Goals for Patients at “Extreme” ASCVD Risk. Curr Diab Rep. 2019 Nov 21;19(12):146.
- Yu X, Yuan Y, Dong X, et al. Low apolipoprotein B and LDL-cholesterol are associated with the risk of cardiovascular and all-cause mortality: a prospective cohort. Ann Med. 2025 Dec;57(1):2529565.
- Nordestgaard BG, Langsted A. Lipoprotein(a) and cardiovascular disease. Lancet. 2024 Sep 28;404(10459):1255-64.
- Available at: https://www.washingtonpost.com/health/2026/01/02/lpa-heart-clinical-trial-treatment/. Accessed February 3, 2026.
- Available at: https://www.managedhealthcareexecutive.com/view/new-therapies-on-the-way-to-lower-lp-a-a-cardiovascular-risk-factor. Accessed February 3, 2026.
- Available at: https://clinicaltrials.gov/study/NCT04023552. Accessed February 3, 2026.
- O’Donoghue ML, Rosenson RS, Gencer B, et al. Small Interfering RNA to Reduce Lipoprotein(a) in Cardiovascular Disease. N Engl J Med. 2022 Nov 17;387(20):1855-64.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun